28
|
Volume3 Issue5
S
upporting
Y
our
P
ractice
bitewing radiographs to ruleout anynew toothdecay
or other conditions. Therewereno significant findings
uponclinical examinationandnocauses for concern
were identified.
It is common for patientsdiagnosedwith
schizophrenia to require readmission tohospital
for stabilizationas a result of non-compliancewith
medicationanddeteriorationof their condition.While
aconcurrent historyof polysubstanceabusemight
haveprecipitated thepatient’s readmission to the
hospital, substanceabusewasnot an issueat this
particular time inhis treatment.
Thepatient toldDr. Clarkhe felt “divided inhalf”
becauseof hisone remainingprimarymolar. The side
withnoprimary teeth felt likeanadult. Theother side,
theonewith the retainedprimary85, renderedhim
feeling likeachildor infant. Hewashavingdifficulty
dealingwith theseconflicting feelings, andhe
indicatedonly feelingable tochewon the “adult” side
of hismouth.
Diagnosis
As the investigationdidnot reveal any significant
clinical findings that couldexplain thepatient’s
discomfortwith tooth85, itwasdetermined that it
was solelyamanifestationof thepatient’sdelusional
thought process.
“Delusions areacommon featureof thepositive
symptomcomplexof schizophrenia,meaning that
theyareobservablewhile they shouldnot be,” explains
Dr. Clark. “Theother two symptomcomplexes are
disorganizedandnegative symptoms. Thispatient
displayedprimarilypositive symptoms inhisoverall
diagnosisof thedisease,whichdoes carryabetter
prognosiswith treatment, andoftenabetter response
toantipsychoticmedications that areprescribed for
thesepatients.”
TreatmentPlan
“Inmyexperience, retainedprimarymolars inadult
patients can survivequitewell formanyyears, and
there’sno indication thatwehave to intervene
andextract them. Theyarean inexpensiveway to
retain spaceandprovide some function—while
perhaps limited for this individual,” saysDr. Clark. He
explained this reasoning to thepatient. “Hewas very
pleasant andhe listenedwhileweexplained thepros
andconsof both tooth retentionandextraction,”
Dr. Clark remembers. “I presentedhimwithmy
recommendations andexplained that I declined to
extract his tooth for the reasons that I had just given
him.While itwasn’twhat hewanted tohear, hewas
acceptingof it.”
Thepatient returned to thedental clinic to see the
hygienist, andwas certainlymotivated to lookafter
his teeth. Hewasdischarged from thehospital shortly
after that time.
a
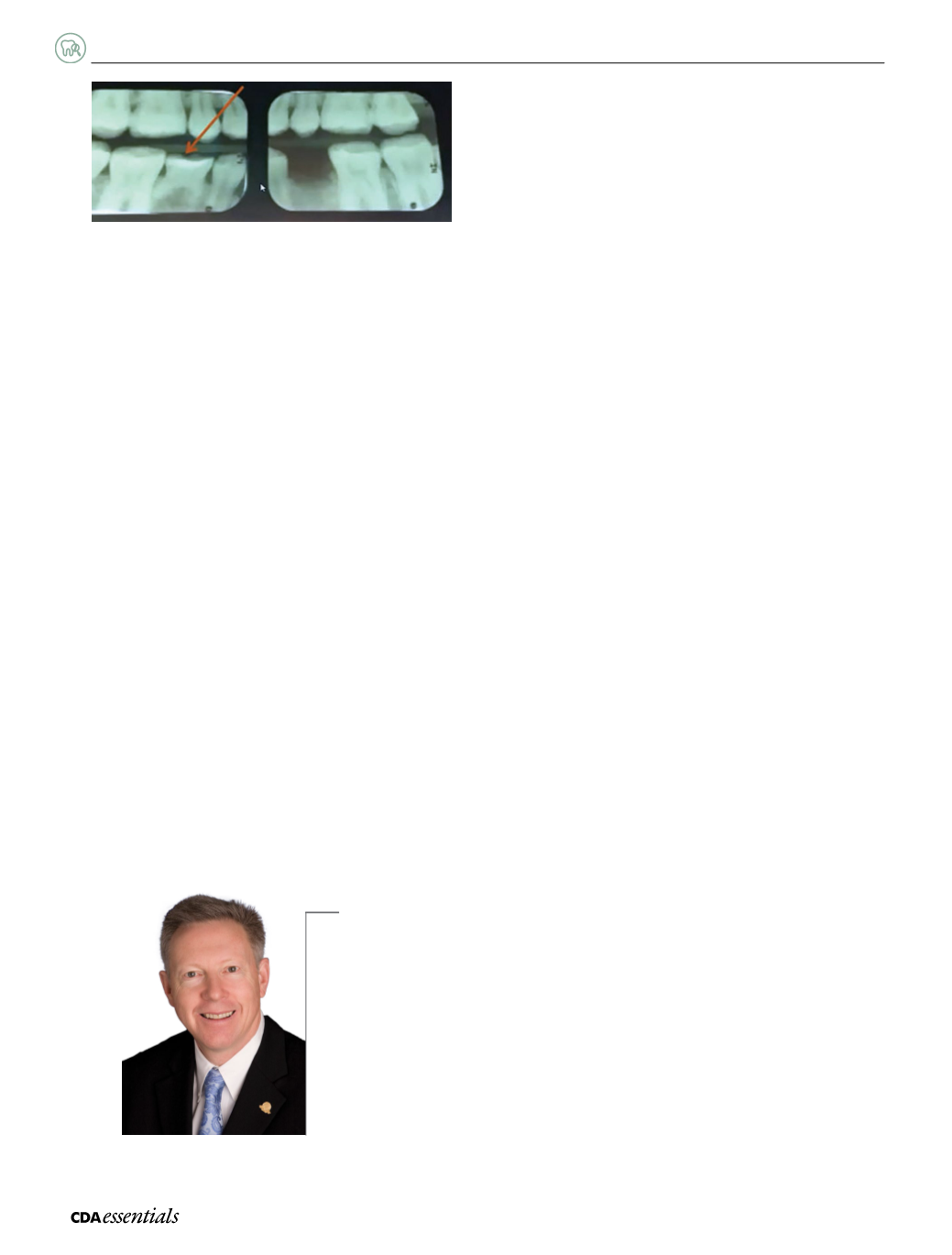
Figure1:
Bitewing radiographs showing thepresence of retained tooth85,
and theabsence of clinical findings explaining thepatient’s concerns.
Could extractionhavebeen the solution?
Could tooth extractionhave eliminated thedelusional thought process? “Sure,we could easilyhave
extracted the tooth,” recognizesDr.Clark. “Yet shouldanotherpractitionerhave later recommended
theuse of an implant oranotherprosthetic replacement, therewouldhavebeen thepotential for it to
trigger furtherdelusional thinkingor thought processes typical of this positive symptom complex.”For
example, thepatient could eventuallyhaveperceived the implant as something foreign tohim. It could
alsohave resulted in thedelusionof thought broadcasting—anothervery commondelusional thought
process that occurs inpatientswith thisdiagnosis—, creatingawholenewareaof conflict for this
patient. “The simplest approach, and the one Iwas quite comfortablewith,was todecline to remove the
tooth forhimat that time,”Dr.Clark concludes.
Dr.DavidClark


