25
Volume3 Issue5
|
I
ssues and
P
eople
Resumecomprehensive riskmanagement care
Printedwithpermissionof IanMcConnachie,DDS,MS,FRCD(C)
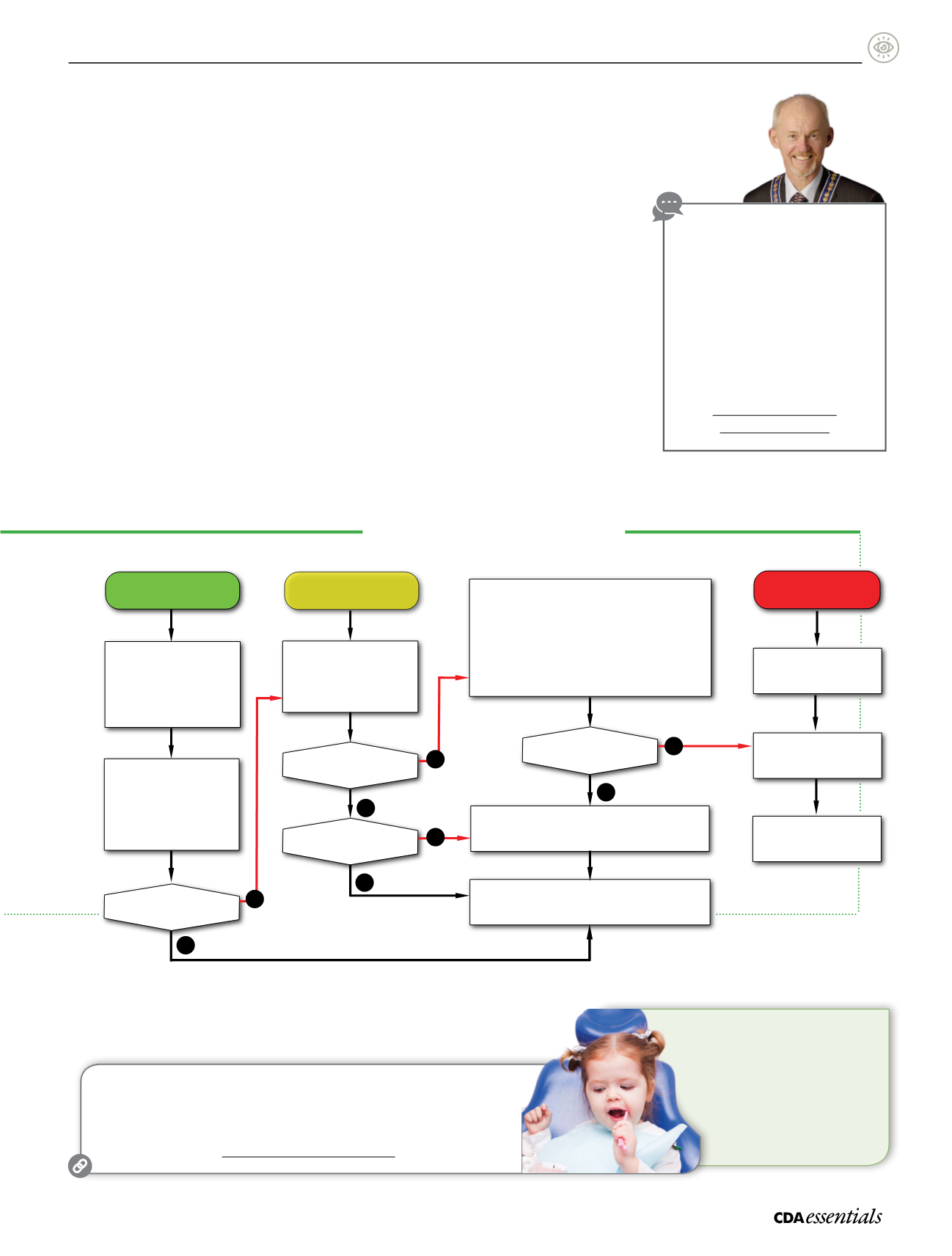
RiskManagementAlgorithm
EarlyChildhoodCaries
AnticipatoryGuidance
Diet
Growthanddevelopment
Commitment toappropriate
periodicityof o cecare
Motivational interviewing
LowRisk
High risk:
cavitated lesions
Moderate tohigh risk:
non-cavitated lesions
Reducedperiodicityand
treatments:
Annual visits
Introduction toprophylaxis
as childdevelopment
progresses
X-rays requiredat a laterdate
Patient statusdeteriorates?
Assess for:
Anti
microbials
–Topical fluoride
–Sealants
–Appropriatep
eriodicity
Patientbecomeshigh risk?
Restorationneed
ed?
Stagedcare:
Systematicdesensitization
Antimicrobials
Topical uoride
–Atraumatic restorative treatment (ART)
Glass ionomer (GI) sealants
Appropriateperiodicity
(May include initial sedationvisit(s) tocontrol painand infection.)
Unstableclinical situation?
Permanent restorationwithorwithout sedation
Stagedcarewhilewaiting
forgeneral anesthesia
*Decision to treator refer cancomeat any stage.
Treatmentunder
general anesthesia
Completionof
restorative treatment
Yes
No
No
No
No
Yes
Yes
Yes
Theelementsof thefirst dental visit arebroadand
build important links:
Parent interview
Assessment of parentalmotivation
Visual exam toassess risk
Development of a riskmanagement protocol
Oral hygiene instructions
Applicationanddispensationof preventive
therapies
“Havingexamined thechildand taken in the
relevant information,wecanposition them into
themost appropriate risk categoryusingone
of theassessmentmodels available,with the
3general categoriesbeing low risk,moderate
tohigh risk (non-cavitated lesions), andhigh risk
(cavitated lesions),” addsDr.McConnachie.
Riskmanagement
“As careproviders,weneed tofirst decidehow
far into thealgorithmwearecomfortablegoing,
andatwhat pointweneed to refer toanother
clinician—and thisobviously includesbuilding
a relationshipwith thepediatric
specialist, consistentwithour
ownphilosophyof care,”
emphasizesDr.McConnachie.
Dr.McConnachieencourages
dentists to take theplunge
and treat youngpatients: “Start
slowly. Get comfortablewith the
lower-riskpatients. Startwith
thefirst exambyfirst birthday.
Build skills. AlwayshaveaplanB,
andbeprepared toenjoy the
experience!”
a
Visit
OasisDiscussions
to
watchavideo interviewwith
Dr.McConnachie.
Thevideo includes anoverview
ofDr.McConnachie’s algorithm
for ECC riskassessment
andmanagement, and
thepresentationof
ECC risk-management cases.
oasisdiscussions.ca
/2015/06/09/eccp
ShareYourExperience
Doyou see infants inyour practice?
Haveyouadopteda riskmanagement approach toECC?
Sendyour feedback to
or call 1-855-716-2747.
Forourreaders inOntario, further informationon
thistopicwasrecently featured inOntarioDentist
magazine:
McConnachie, I.Newsolutions forgeneral
practitioners intreatingearlychildhoodcaries.
OntarioDentist.2016;93(2):23-25.
McConnachie, I.Stagedcare–newsolutions
fortreatingearlychildhoodcaries.
OntarioDentist.
2016;93(3):32-36.


