














 32 / 48
32 / 48

32
|
Volume 2 Issue 5
S
upporting
Y
our
P
ractice
Send us your comments
or clinical questions.
oasisdiscussions@cda-adc.caor use the CDAOasis App.
Antibiotic Therapy in
Revascularization/Revitalization
The use of antibiotic mixtures as intracanal
medicaments to cleanse and “sterilize” the
canal has become increasingly popular.
The necrotic tooth is commonly filled
with a combination of metronidazole,
ciprofloxacin and minocycline. After
3 months, the canal is accessed again,
bleeding is induced to fill the canal with
blood, and the canal is sealed with a
collagen plug, MTA and then amalgam.
The blood clot creates a biological scaffold
to aid in the growth of new tissue within
the canal space. Additionally, the growth
and differentiation factors within the blood
clot support the healing process. More
recently, some techniques utilize blood that
is drawn from the patient and centrifuged
to isolate platelet-rich plasma (PRP) or
plasma-rich growth factor (PRGF), which is
then injected into the canal. Although the
treated tooth appears radiographically to
develop a typical root shape, animal studies
suggest that the new tissues are not dentin
and pulp but rather cementum with bony
islands and connective tissue (see
➌
,
➍
).
a
Theviewsexpressedarethoseoftheauthorsanddonotnecessarilyreflectthe
opinionsorofficialpoliciesoftheCanadianDentalAssociation.
References
1.BansalR,JainA,MittalS,KumarT,KaurD.Regenerativeendodontics:
aroad lesstravelled.
JClinDiagnRes.
2014;8(10):ZE20-4.
2.BakhtiarH,VatanpourM,RayaniA,NaviF,Asna-AshariE,AhmadiA.,et
al.Theplasma-rich ingrowth factorasasuitablematrix inregenerative
endodontics:acaseseries.
NYStateDentJ.
2014;80(4):49-53.
3.CemGüngörHC,UysalS,AltayN.Aretrospectiveevaluationofcrown-
fracturedpermanentteethtreated inapediatricdentistryclinic.
Dent
Traumatol.
2007;23:211-7.
4.ShabahangS.Treatmentoptions:apexogenesisandapexification.
Pediatr
Dent.
2013;35(2):125-8.
5.ThibodeauB,TropeM.Pulprevascularizationofanecrotic infected
immaturepermanenttooth:casereportandreviewofthe literature.
Pediatr
Dent.
2007;29(1):47-50.
6.Cvek,M.Treatmentofnon-vitalpermanent incisorswithcalcium
hydroxide. I.Follow-upofperiapicalrepairandapicalclosureof immature
roots.
OdontolRevy.
1972;23(1):27-44.
7.WangX,Thibodeau,B,TropeM,LinHM,HuangGT.Histologic
characterizationofregeneratedtissues incanalspaceafterthe
revitalization/revascularizationprocedureof immaturedogteethwith
apicalperiodontitis.
JEndod.
2010;36(1):56-63.
THE AUTHORS
Dr.Michael Casas
Dr. Casas is an associate
professor in the faculty of
dentistry at the University
of Toronto and director
of dentistry clinics at
The Hospital for Sick
Children.
Dr. SuhamAlexander
Dr. Alexander is in
private practice in Ottawa
and is a clinical editor
for Oasis Discussions at
CDA.
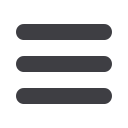
Radiographic view at 18 months
follow-up, demonstrating
narrowing of root canal in the
apical third and thickening of
the lateral walls. A normal bony
architecture at the periradicular
region is evident.
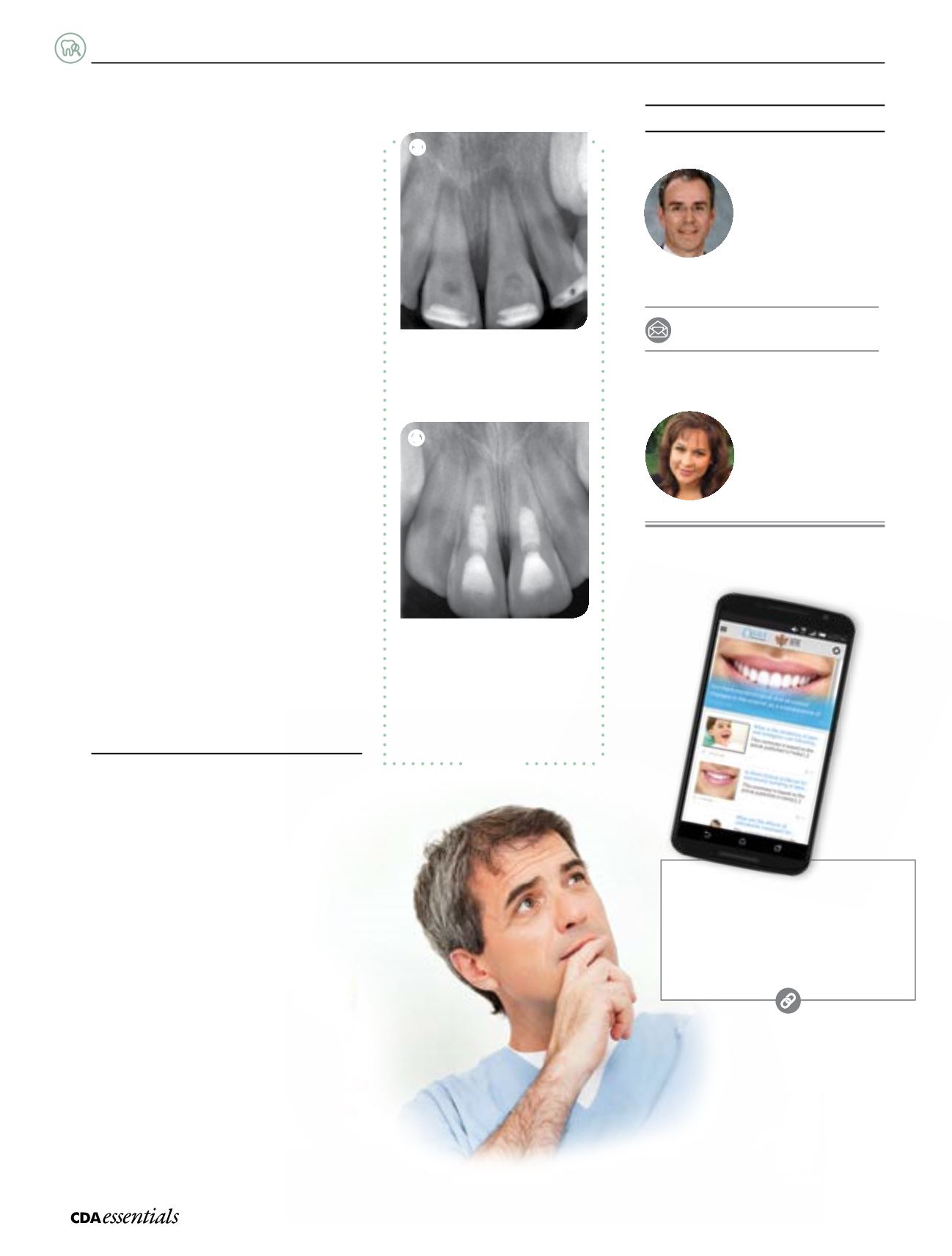
Radiographic view after intracanal
application of calcium hydroxide
paste; periradicular radiolucencies
are evident in both roots.
➌
➍
michael.casas@sickkids.caCase 2