
![]()
![]()
Bilateral Dentigerous Cysts - Report of an Unusual Case and Review of the Literature
K. S.C. Ko, DDS
D.G. Dover, DDS, MRCD(C)
R.C.K. Jordan, DDS, M.Sc., PhD, FRCD(C)
ABSTRACT
Dentigerous cysts are the most common developmental cysts of the jaws, most frequently
associated with impacted mandibular third molar teeth. Bilateral dentigerous cysts are
rare and occur typically in association with a developmental syndrome. The reported
occurrence of bilateral dentigerous cysts in the absence of a syndrome is rare and, to
date, only 11 cases have been described. Here, we report a case of bilateral nonsyndromic,
dentigerous cysts and review the literature for this unusual finding.
MeSH Key Words:
case report; dentigerous cyst/pathology; mandibular diseases/pathology.
© J Can Dent Assoc 1999; 65:49-51
This article has been peer reviewed.
[Introduction | Case Report | Radiographic Findings | Treatment | Pathology | Discussion | Reference]
A dentigerous cyst is an epithelial-lined developmental cavity that encloses the crown of an unerupted tooth at the cementoenamel junction. Dentigerous cysts are the second most common odontogenic cysts after radicular cysts, accounting for approximately 24% of all true cysts in the jaws.1 Their frequency in the general population has been estimated at 1.44 cyst for every 100 unerupted teeth.2 The cyst arises from the separation of the follicle from the crown of an unerupted tooth, and although it may involve any tooth, the mandibular third molars are the most commonly affected.
Dentigerous cysts are frequently discovered when radiographs are taken to investigate a failure of tooth eruption, a missing tooth or malalignment. There is usually no pain or discomfort associated with the cyst unless it becomes secondarily infected. Radiographs show a unilocular, radiolucent lesion characterized by well-defined sclerotic margins and associated with the crown of an unerupted tooth. While a normal follicular space is 3 to 4 mm, a dentigerous cyst can be suspected when the space is more than 5 mm.3
Most dentigerous cysts are solitary. Bilateral and multiple cysts are usually found in association with a number of syndromes including cleidocranial dysplasia and Maroteaux-Lamy syndrome.4 In the absence of these syndromes, bilateral dentigerous cysts associated with the mandibular third molars are rare. To date, there have been only 11 reported cases in the literature (Table I).5-15 Here, we report the unusual occurrence of nonsyndromic bilateral dentigerous cysts associated with mandibular third molars.
Authors |
Year |
Sex |
Race |
Age (yrs.) |
Location |
Treatment |
Sands and Tocchio5 |
1998 |
F |
N/A |
3 |
Md. central incisors and first molars |
Enucleation |
Banderas and others6 |
1996 |
M |
C |
38 |
Md. third molars |
Enucleation |
O’Neil and others7 |
1989 |
M |
Bl |
5 |
Md. first molars |
Enucleation |
Eidinger8 |
1989 |
M |
C |
15 |
Md. first molars |
Enucleation |
McDonnell9 |
1988 |
M |
N/A |
15 |
Md. second premolar and second molar teeth |
Enucleation |
Crinzi10 |
1982 |
F |
Bl |
15 |
Md. third molars |
Enucleation |
Swerdloff and others11 |
1980 |
F |
C |
7 |
Md. first molars |
Enucleation |
Burton and others12 |
1980 |
F |
Bl |
57 |
Md. third molars |
Enucleation |
Callaghan13 |
1973 |
M |
C |
38 |
Md. third molars |
Enucleation |
Stanback14 |
1970 |
M |
N/A |
9 |
Md. first molars |
Enucleation |
Myers15 |
1943 |
F |
N/A |
19 |
Md. third molars |
Enucleation |
N/A= Not available
M = male
C = Caucasian
F = female
Bl = Black
Md. = mandibular
A 42-year-old Caucasian man was referred to the department of dentistry of the Sunnybrook Health Science Centre by an outside emergency dental service for the evaluation of an asymptomatic, cystic lesion in the right mandible. Intraoral examination revealed an extensively restored dentition and clinically absent third molar teeth. No extraoral swellings or tenderness in relation to the mandibular third molars was noted. The patient's medical history was nonsignificant except for a case of bronchitis and chronic fatigue. There were no associated syndromes present.
A panoramic radiograph showed absent upper third molars. Bilateral, unilocular well-defined corticated radiolucencies surrounding both unerupted mandibular molars were identified. The anterior border of both radiolucencies appeared to involve the distal root of the second molar (Fig. 1). Both third molars were grossly displaced to the inferior border of the mandible.
 |
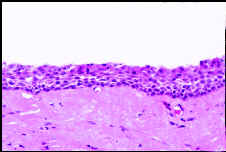 |
| Fig.1 Preoperative panoramic radiograph showing bilbateral well-defined radiolucencies involving both un-erupted mandibular third molar teeth. | Fig.2 Photomicrograph showing cyst wall composed of fibrous tissue and lined by nonkeratinised stratified sqaumour epithelium.(H& E X 40) |
Treatment
The clinical diagnosis was bilateral dentigerous cysts. Under general anesthesia, the buccal flaps were raised and the cysts enucleated together with the associated third molar teeth. Healing was uneventful, and one week after the operation, the surgical sites showed good healing. There was partial paresthesia on the left side affecting the mental nerve distribution of the inferior alveolar nerve, but after three months, there had been complete healing. There was also no evidence of recurrence of the cysts.
The submitted specimen consisted of two sacs of soft tissue, the largest measuring 30 x 7 x 5 mm. Microscopic sections of both specimens were similar, showing cyst walls composed of fibrous tissue and lined by stratified squamous, non-keratinized epithelium with Rushton bodies (Fig.2).
Discussion
Although dentigerous cysts are common developmental cysts, reported bilateral dentigerous cysts are extremely rare. Bilateral or multiple dentigerous cysts are usually associated with the Maroteaux-Lamy (mucopolysaccharidosis, type VI) syndrome16 and cleidocranial dysplasia.17 Both are developmental conditions that are detected in young individuals with stigmata of the syndromes.
Maroteaux-Lamy syndrome is one of the mucopolysaccharidoses (MPS), a group of diseases resulting from a genetic defect in the degradation of specific mucopolysaccharides. With this syndrome, there is a deficiency of N-acetyl-4-sulphatase that results in impaired degradation of dermatan sulphate, which accumulates in tissues and is excreted in the urine. Dental features include unerupted dentition, dentigerous cysts, malocclusions, condylar defects, and gingival hyperplasia.16 Cleidocranial dysplasia is an autosomal dominantly inherited disorder that results in a partial or complete absence of clavicles, short stature, frontal and parietal bossing, maxillary micrognathia, prolonged retention of the primary dentition, delayed eruption of the permanent dentition, and unerupted supernumerary teeth.17 Multiple dentigerous cyst formation occurs in both conditions and can develop at any site in the upper or lower jaws.
Bilateral dentigerous cysts are rare in the absence of an underlying syndrome or systemic disease. An extensive search of the English language literature has identified only the 11 cases reported in Table I. Although this finding may reflect the true rarity of the condition, it is conceivable that bilateral dentigerous cysts are either under-recognized or under-reported.
The age range for the reported cases varies widely, from 5 to 57 years of age. Four of the cysts occurred in children under the age of 12. All but three cases6,12,13 were identified at ages corresponding to the normal eruption times of the affected teeth. As with our case, these three cases occurred in asymptomatic individuals, which accounts for the delayed diagnosis. All but two of the 11 cases5,9 have been associated with mandibular molar teeth, with five of these associated with the third molar teeth.6,10-13 There have been no reported cases of nonsyndromic, bilateral dentigerous cysts occurring in all four dental quadrants.
Since cysts can attain considerable size with minimal or no symptoms, early detection and removal of the cysts is important to reduce morbidity. Moreover, all but one11 of the reported cases, including ours, presented without pain. And, all but one were discovered during investigation of asymptomatic slow-growing swellings.11
It is therefore important to perform radiographic examination of all unerupted teeth. While bite-wing and periapical radiography is typically performed in the routine examination of patients with a healthy dentition, this series of radiographs may occasionally fail to delineate the full extent of a lesion if present. A panoramic radiograph supplemented with skull series or more advanced imaging such as tomography may permit a better delineation of the extent of the lesion and its relationship to adjacent anatomical structures.
Dr. Ko was a dental resident, department of dentistry, Sunnybrook Health Science Centre, Toronto, Ont.
Dr. Dover is an oral and maxillofacial surgeon, department of dentistry, Sunnybrook Health Science Centre, Toronto, Ont.
Dr. Jordan is an oral pathologist, department of dentistry, Sunnybrook Health Science Centre, and in the department of laboratory medicine, Sunnybrook Health Science Centre, Toronto, Ont.
Reprint requests to: Dr. Richard Jordan, H-126, Sunnybrook Health Sciences Centre, 2075 Bayview Ave., Toronto ON M4N 3M5.
1. Daley TD, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Sur Oral Med Oral Patho 1994; 77:276-80.
2. Mourshed F. A roentgenographic study of dentigerous cysts. I. Incidence in a population sample. Oral Surg Oral Med Oral Pathol 1964; 18:47-53.
3. Goaz PW, Stuart CW. Cysts of the jaws. In: Oral radiology, principles and interpretation. 3rd ed. St. Louis: Mosby; 1994. p. 400.
4. Gorlin RJ. Cysts of the jaws, oral floor and neck. In: Gorlin RJ, Goodman HW, editors. Thoma's oral pathology. 6th ed. St. Louis: Mosby; 1970. Vol. 1.
5. Sands T, Tocchio C. Multiple dentigerous cysts in a child. Oral Health 1998; 88(5):27-9.
6. Banderas JA, Gonzalez MA, Ramirez F, Arroyo A. Bilateral mucous cell containing dentigerous cysts of mandibular third molars: Report of an unusual case. Arch Med Res 1996; 27:327-9.
7. O'Neil DW, Mosby EL, Lowe JW. Bilateral mandibular dentigerous cysts in a five-year-old child: Report of a case. ASDC J Dent Child 1989; 56:382-4.
8. Eidinger GB. Bilateral cysts in the child patient. Report of a case and review of the literature. Univ Tor Dent J 1989; 2:20-3.
9. McDonnell DG. Bilateral dentigerous cysts. A case history. J Ir Dent Assoc 1988; 34:63.
10. Crinzi RA. Bilateral dentigerous cysts of the mandible. Oral Surg Oral Med Oral Pathol 1982; 54:367.
11. Swerdloff M, Alexander SA, Ceen, RF, Ferguson FS. Bilateral mandibular dentigerous cysts in a seven-year-old child. J Pedod 1980; 5:77-84.
12. Burton DJ, Sheffer RB. Serratia infection in a patient with bilateral subcondylar impacted third molars and associated dentigerous cysts: Report of a case. J Oral Surg 1980; 38:135-8.
13. Callaghan JH. Bilateral impaction of lower third molars in association with bilateral dentigerous cyst formation. A case report. Glasgow Dent J 1973; 4:36-8.
14. Stanback JS. The management of bilateral cysts of the mandible. Oral Surg Oral Med Oral Pathol 1970; 30:587-91.
15. Myers PB. Bilateral dentigerous cysts of the mandible. Brit Dent J 1947; 74:67-8.
16. Roberts MW, Barton NW, Constantopoulos G, Butler DP, Donahue AH. Occurrence of multiple dentigerous cysts in a patient with the Maroteaux-Lamy syndrome (Mucopolysaccharidosis, type VI). Oral Surg Oral Med Oral Pathol 1984; 58:169-75.
17. Trimble LD, West RA, McNeill RW. Cleidocranial dysplasia. Comprehensive treatment of the dentofacial abnormalities. J Am Dent Assoc 1982; 105:661-6.