|
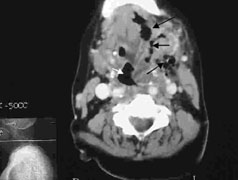
| Figure 1: CT scan with intravenous contrast of the neck. The edge of the mandible is seen anteriorly and the vertebrae posteriorly. The airway (at the level of the epiglottis) is deviated severely to the left (white arrow). Gas bubbles are seen in the soft tissue to the right (black arrows). |
 |
| Figure 2: CT scan with intravenous contrast of the chest. The aortic arch is seen anteriorly with the trachea and esophagus posteriorly. Streaking of the fat plane between the aorta and sternum is indicative of infection (black arrow). |
 |
| Figure 3: Planned incisions of the neck. The incision to the right is along the sternomastoid and was used for access to the mediastinum. |
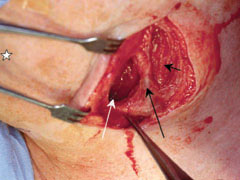 |
| Figure 4: Opening into the neck with a view of the thoracic inlet (white arrow), the external jugular vein (long black arrow) and the sternomastoid muscle (short black arrow). The chin is marked with a star. |
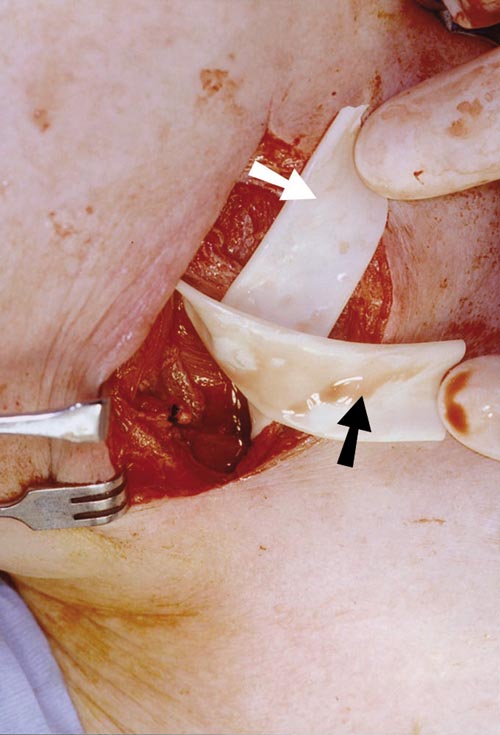 |
| Figure 5: Penrose drains in the submandibular space (black arrow) and the retropharyngeal space (white arrow). |
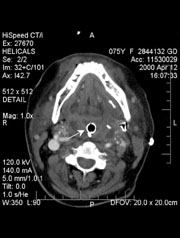 |
| Figure 6: Postoperative CT scan with contrast showing complete obliteration of the airway around the endotracheal tube (white arrow). |
Swelling of the floor of the mouth
Difficulty swallowing
Difficulty talking
Pain while swallowing or pain out of proportion to swelling
Trismus out of proportion to swelling
Stridor (a raspy noise while breathing)
Tracheal deviation
Inability to tolerate secretions
Swollen tongue
Raised tongue or floor of mouth
Muffled voice (“hot potato” voice)