• Harinder S. Sandhu, DDS, PhD, Dip. Perio. •
Abstract
MeSH Key Words: counselling; dentists; tobacco use cessation; tobacco use disorder/drug therapy
© J Can Dent Assoc 2001; 67:153-7
Despite public knowledge of morbidity caused by tobacco use, 25-30% of Canadian and U.S. citizens continue to use tobacco.3,7 There are indications that the incidence of new, young smokers, especially females, is on the rise.8 The pub licity caused by high-profile court cases in the United States has made people more aware of the dangers of smoking, and covert attempts by tobacco companies to hide the deleterious effects of smoking have further sensitized the public and health care professionals to the issue.
Counselling by health professionals is an effective method in guiding patients toward smoking cessation.9 A large proportion of the general public, including smokers, visit the dental office regularly.10,11 Thus, it seems imperative that dental offices should be involved in smoking cessation efforts.
This paper discusses various issues surrounding tobacco use and provides a step-by-step approach that dental offices can use to guide patients in eliminating tobacco use.
Nicotine Dependency Nicotine addiction should be treated as a chronic disease. The majority of patients who make an initial attempt to quit will continue to use tobacco and to cycle through periods of relapse and remission.12 Tobacco dependency is a serious addiction, a complex biopsychosocial phenomenon in which genetics, pharmacology, psychology, and environment interact to produce chronic and tenacious drug use. Unless the biophysiological, behavioural, spiritual, and social components of this dependency are addressed, the health care professional will be frustrated in counselling patients addicted to tobacco. The link between environmental stimuli and the quick and pleasurable effect of smoking makes quitting very difficult. The clinician must address the patient’s fear of withdrawal symptoms. Psychological and emotional triggers are very much connected with the smoking habit, and therefore patients must be counselled to cope with moments of temptation through the development of alternative strategies. The smoker’s self-image and socialization behaviour must be changed to accommodate the new self-awareness of a smoke-free person.12
Clinical Tobacco Intervention in the Dental Office
Create a Smoke-Free Environment
All dental staff should attend an accredited tobacco cessation program. These programs are available through local health units as well as through universities as continuing education courses. In Ontario, they are available through the Ontario Dental Association (ODA) and the Ontario Medical Association (OMA). Staff training will ensure that tobacco intervention strategies are standardized and that patients get the same message from all personnel. If one member of the staff is trained, then other staff can be trained in-house.
Any dental staff member using tobacco should be helped and encouraged to quit. A member who smokes will have no credibility in advising patients.
Patient Assessment Medical and dental history charts should include questions about tobacco use and should document how long the patient has been smoking and how much he or she smokes (mild addiction, 1-5 cigarettes per day; moderate addiction, up to 10 cigarettes per day; severe addiction, up to 20 or more cigarettes per day).
A more precise evaluation of the level of dependency can be done using the Fagerström test.13 This test is scored on a 4-point scale. The questions ask about the time to the first cigarette of the day and previous history of withdrawal symptoms. The test also assesses the patient’s ability to resist the urge to smoke when he or she may be in areas where smoking is not allowed or when the patient has been ill. The higher the score, the more severe the dependency.
Strategies The strategies used in clinical tobacco intervention depend on the user’s level of addiction. Patients who do not smoke, especially young patients, should be complimented and encouraged never to begin.
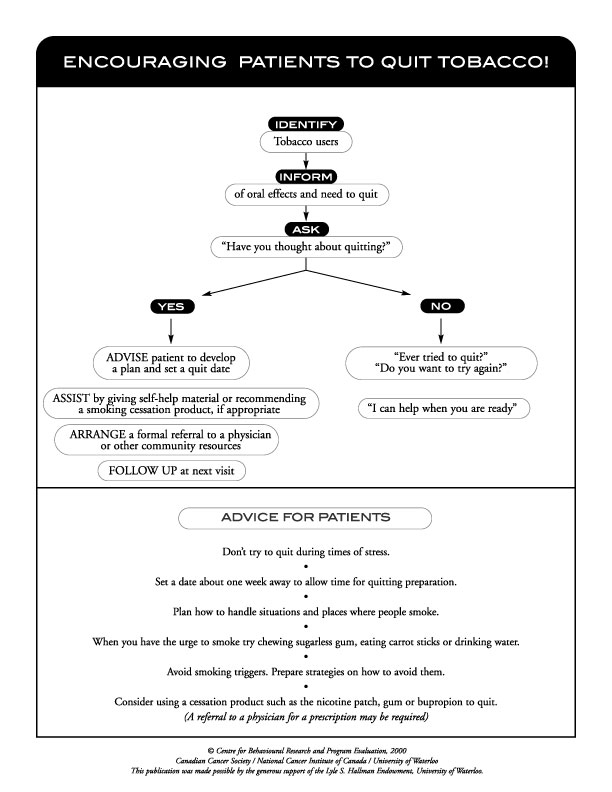
As for smokers, a quick assessment should be made of each patient’s current desire to quit smoking. Steps for this assessment are listed in Fig. 3. (For further information on stages of change, readers are encouraged to consult the article by Prochaska and DiClemente.14)
Patients who smoke should be advised of the effects of smoking on general health and on oral health, specifically. In doing so, it is helpful to have pictures of non-smokers and smokers to compare as well as pictures of patients whose oral health has improved following smoking cessation.
Therapeutic Goals and Intervention Dentists and dental hygienists should check the status of patients’ tobacco use at every visit and continue to provide current information. Patients who are not ready to quit should be asked to at least consider tobacco cessation. Patients must not feel as if they are being pressured, but should be encouraged and offered help in making the final decision to quit. Counselling based on the stages of behavioural change has been successfully applied in tobacco cessation treatment.16 Brief interventions of 3 to 4 minutes can move patients through these various stages.12,16 Rather than pressuring patients into immediate, radical changes, dental staff should try to move the patients through one stage at a time. A brief description of the therapeutic goals and interventions linked to each stage appears in Table 1. In Ontario, the OMA and the ODA offer information to their members who wish to act as smoking cessation counsellors.
Different levels of addiction should be treated differently.16 Although clinical and epidemiological evidence indicates that more intense therapies have higher success rates,16 mild smokers may not need such intensive therapies. The following are decision-making guidelines regarding tobacco cessation interventions:
• mild level of addiction: brief behavioural inter vention; NRT
• moderate level of addiction: brief behavioural intervention; NRT; adjunctive pharmacotherapy
• severe level of addiction: brief behavioural intervention; NRT; adjunctive pharmacotherapy; intensive behavioural therapy.
Pharmacotherapy Only about 3 to 4% of patients are success ful when they try to quit without help. It is estimated that this rate could be doubled with counselling and behavioural modification. Pharmacotherapy can increase the success rate to 30% and should be part of any clinical tobacco intervention program.15,16 Table 2 provides an overview of nicotine replacement therapy (NRT) and adjunct pharmacotherapy use, while Table 3 describes dosages and side effects.
A Word of Caution In Ontario, the Royal College of Dental Surgeons of Ontario (RCDSO) has recognized that the scope of practice of dentistry includes the ability for dentists to prescribe non-NRT medications for their patients as part of a smoking cessation intervention. However, information from the RCDSO to its members indicates that dentists who wish to become involved in such patient care should first complete appropriate training. For example, a thorough knowledge of the mechanisms of action of various non-NRT medications and their side effects should be obtained through a recognized training program.
Many dentists may still not feel qualified to prescribe some of the non-NRT medications and are advised to consult with their patient’s family physician. This is particularly important as the pharmacokinetics of certain medications may change, with or without nicotine replacement, as a result of smoking cessation.12 The dosage of certain medications may therefore require adjustment. There is a great deal of misinformation currently circulating regarding the use of NRT and non-NRT medications in tobacco cessation programs. The OMA’s Committee on Drugs and Pharmacotherapy has published an excellent paper on myths and facts about pharmacotherapy cessation programs.18 Some of these facts are summarized in Table 4.
Intensive Behavioural Change Dental professionals should limit themselves to brief interventions or counselling sessions. Heavy tobacco users, particularly those with co-morbidity-like clinical depression and advanced social and emotional conflicts, will require intensive behavioural interventions. These patients should be referred to family practice clinics dealing with addiction issues or be treated by clinical psychologists or psychiatrists.
Relapse Prevention The majority of patients who attempt to quit smoking will relapse. Generally many attempts are required to quit smoking. Relapse is often a natural part of the quitting process. Patients should be encouraged to learn from relapses and to develop strategies to avoid them in future attempts. Patients should be encouraged by statements like, “Now you know that you can quit smoking: you have already been smoke-free for 3 weeks.” Patients should be advised to abstain from consuming alcohol, to avoid stressful and emotional situations, and to avoid attending social functions or gatherings where others may be smoking. Socializing in the work-place, where there may be other smokers, is hard to avoid.
Acknowledgments: The author wishes to thank Dr. Diane Midmer for her permission to use information from the Smoking Cessation Module at Project Create.
Dr. Sandhu is professor and chair , division of periodontology, faculty of medicine and dentistry, The University of Western Ontario.
Correspondence to: Dr. Harinder S. Sandhu, Division of Periodontology, School of Dentistry, The University of Western Ontario, London, ON N6A 5C1. E-mail: hsandhu@julian.uwo.ca
The author has no declared financial interest. The views expressed are those of the author and do not necessarily reflect the opinion or official policies of the Canadian Dental Association.
References 1. Bartecchi CE, MacKenzie TD, Schrier RW. The human costs of tobacco use (1). N Engl J Med 1994; 330(13):907-12.
2. MacKenzie TD, Bartecchi CE, Schrier RW. The human costs of tobacco use (2). N Engl J Med 1994; 330(14): 975-80.
3. Health Canada. National population health survey highlights: smoking behaviour of Canadians. Cycle 2, 1996/97. Fact sheet 1, 2. Overview of results. Ottawa, 1999.
4. Position paper: tobacco use and the periodontal patient. Research, Science and Therapy Committee of the American Association of Periodontology. J Periodontol 1999; 70(11):1419-27.
5. Bastiaan RJ, Reade PC. The effect of tobacco smoking on oral and dental tissues. Aust Dent J 1967; 21(4):308-15.
6. Bain CA, Moy PK. The association between the failure of dental implants and cigarette smoking. Int J Oral Maxillofac Implants 1993; 8(6):609-15.
7. Garfinkel L. Trends in cigarette smoking in the United States. Prev Med 1997; 26(4):447-50.
8. Tobacco use among high school students - United States, 1997. MMWR Morb Mortal Wkly Rep 1998; 47(12):229-33.
9. Physicians and other health-care professional counseling of smokers to quit - United States, 1991. MMWR Morb Mortal Wkly Rep 1993; 42(44):854-7.
10. Tomer SL, Husten CG, Manley MW. Do dentists and physicians advise tobacco users to quit? J Am Dent Assoc 1996; 127(2): 259-65.
11. Campbell HS, Sletten M, Petty T. Patient perceptions of tobacco cessation services in dental offices. J Am Dent Assoc 1999; 130(2):219-25.
12. Project CREATE: Volume 3, Smoking Cessation: Published by Project CREATE: University of Toronto, 1998.
13. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire. Br J Addict, 1991; 86(9):1119-27.
14. Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol 1983; 51(3):390-5.
15. Fiore MC, Smith SS, Jorenby DE, Baker TB. The effectiveness of the nicotine patch for smoking cessation. A meta-analysis. JAMA 1994; 271(24):1940-7.
16. A clinical practice guideline for treating tobacco use and dependence: A US Public Health Service report. The Tobacco Use and Dependence Clinical Practice Guideline Panel, Staff, and Consortium Representatives. JAMA 2000; 283(28):3244-54.
17. Bupropion (Zyban) for smoking cessation. Med Lett Drugs Ther 1997; 39(1007):77-8.
18. Rethinking Stop-Smoking Medications: myths and facts. Ontario Medical Association Health Policy Department 1999.
{kind=link}
{kind=link}