• George Freedman, DDS, FAACD •
• Fay Goldstep, DDS •
• Tomas Seif, DDS, MS •
• Jaffar Pakroo, DD
© J Can Dent Assoc 1999; 65:579-81
[Early Detection and Treatment |Ultraconservative Preparation|The Ultraconservative Technique|Summary |References]
Natural enamel and dentin are still the best “dental materials” in existence; therefore, minimally invasive procedures that conserve a greater part of the natural, healthy tooth structure must be considered desirable. Minimally invasive procedures are beneficial from a patient’s standpoint as well. There is less discomfort and less need for local anesthesia. There is also a real prospect that the repaired natural tooth will last a lifetime. The replacement of amalgam restorations leads to larger restorations that have shorter life spans, and the replacement procedures themselves may cause damage to adjacent healthy teeth.
In many parts of the world, restorative dentistry has been called conservative dentistry. It has hardly been conservative of tooth structures, however, as traditional methods have been highly invasive and have required the removal of otherwise healthy enamel and dentin.
Fortunately, the current era of dentistry has brought with it new materials, techniques and instruments that make conservative dentistry practical and ultraconservative dentistry a reality. Adhesive restorations eliminate the need for more extensive retentive preparations. Enamel-like composites (both hybrid and flowable) offer long-lasting tooth structure replacement with minimum requirements for bulk. Early detection and ultraconservative restoration prevent secondary caries. New instruments such as microabrasion devices and fissurotomy burs offer the dentist techniques that permit minimal preparation and maximum patient acceptance.
Over the past several decades, there has been a major change in the pattern of dental decay due largely to the increased education of the public and more frequent preventive care by dentists. Consequently, caries incidence is lower and cavities are smaller, particularly among the younger age groups.
While this change represents great progress for the dental profession, it has resulted in some new questions being raised:
1. How can the practitioner effectively diagnose these much smaller lesions in the teeth?
2. Should these smaller lesions be left to grow larger for easier diagnosis and access or should they be intercepted while they are still small?
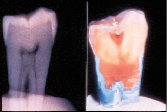 |
| Figure 1: Carious lesion not visible on radiography but seen on cross-section of the tooth. |
Minute lesions may be quite difficult to diagnose with traditionally accepted techniques. The shape of pit and fissure lesions tends to mask the defect when the dentist is using an explorer, as the narrow occlusal opening prevents the entry of the instrument into the lesion. Histologic cross-section has confirmed a ratio of 1:4 (25%) accuracy in diagnosing decay underlying the occlusal surface using the traditional explorer method.1
Radiographs can detect caries when none are observed clinically, but all too often there are caries present in the tooth that the radiograph will not reveal (Fig. 1). This problem is known as hidden caries.2-4
The dilemma of diagnosing these small carious lesions at an early stage is a very real problem that cannot easily be solved by existing diagnostic techniques.5-7 Further complicating this dilemma is the aggressive use of fluoride in fluoridated communities. The surface-hardening effect of fluoride on the enamel makes the tooth surface more impenetrable to exploration, thus masking the carious activity occurring just below the surface and along the dentino-enamel junction (DEJ).
The dentist is faced with having to watch and wait for early caries to become bigger and destroy more healthy tooth structure, or to aggressively eliminate these early lesions and restore the cavities with ultraconservative restorations.
The practice of sealing pits and fissures has enjoyed widespread acceptance.8-10 There has been continued concern, however, about the placement of sealants over undiagnosed caries. Since it is often difficult to determine caries activity in fissures, an exploratory technique or excisional biopsy offers the best diagnostic and conservative technique for the maximum retention of healthy tooth structure combined with the certain removal of all decay. The excisional bur remodels the anatomy of the fissure, facilitating the access, acid etching and bonding of the composite resin into the cavity preparation.11
If this procedure can be accomplished with minimal patient discomfort and without anesthetic, patient acceptance will be high and the dentist’s conservative goals attained.
The goals of ultraconservative preparation are to:
• recontour the fissure and pit anatomy for access and visibility
• explore the cavity to ensure no decay remains
• remove caries ultraconservatively (but completely).
The practitioner has several choices of ultraconservative treatment approaches.
Small Round Burs
While these familiar burs provide conservative preparation and good explorer access, they are slow and inefficient in cutting through enamel. Local anesthetic is often required and the shape of the preparation will leave undercut enamel. However, their use requires no learning curve.
Air Abrasion
 |
| Figure 2: Fissurotomy cutting bur (left) and two polishing burs. |
In recent years, many dentists have begun working with air abrasion technology for the preparation of cavities. Air abrasion allows conservative removal of tooth structure and good explorer access into the preparation with minimal local anesthetic. There is, however, a learning curve associated with these devices in terms of direction, cutting depth and focus of spray since, unlike burs, there is no tactile feedback during the preparation process. Most air abrasion procedures are rather messy as the excess abrasive tends to spread around the operatory. The equipment may be expensive.
Excisional Biopsy Burs
These burs are fast-cutting, conservative and inexpensive, and are specifically designed for recontouring the fissures and accessing decay with minimal enamel removal (Fig. 2). These instruments are familiar to every dentist. In most cases, no anesthetic is required during the entire procedure. Fissurotomy burs are limited to pits, fissures and grooves.
The fissurotomy bur is a new approach to ultraconservative dental treatment. The shape and size of the bur are designed specifically for the purpose of treating pit and fissure lesions. The head length is 2.5 mm, allowing the dentist to control the bur tip to cut just below the DEJ and no further. The tapered shape of the bur allows the cutting tip to encounter very few dentinal tubules, and has been designed to minimize heat build-up and vibration. Since the use of the fissurotomy bur is restricted to enamel, patient discomfort is minimized and the need for local anesthetic eliminated. The design of the fissurotomy bur allows for less invasion than a regular 330 bur (Fig. 3). Traditional cutting burs remove far more enamel at any depth of cut and are designed to access caries that has progressed well beyond the DEJ.
 |
| Figure 3: Traditional 330 bur (left) and anatomically designed fissurotomy bur (right). |
The cavity preparation must be matched with suitable restorative materials. The closest direct material to enamel is composite resin. Since the typical fissurotomy preparation is very narrow, long and irregularly deep, it is important that the restorative material flow easily into all the nooks and crannies. The dental material of choice is a flowable composite. While hybrid composites are stronger and more wear-resistant, it may be difficult to ensure their penetration into the intricate geometry of the narrow preparation to eliminate all the bubbles and gaps. Packable composites are even more technique sensitive in very small cavities.
The Fissurotomy Kit (SS White, Lakewood, NJ) includes Heliomolar Flow (Ivoclar North America, Amherst, NY), a well-established flowable microfill. This composite flows readily into all the crevices of the prepared tooth and adapts to any existing adhesive-bonded internal anatomy. It is also easy to polish.
The Ultraconservative Technique
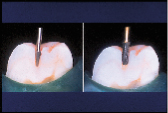
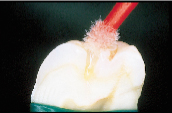
1. Probe all pit and fissure areas. While there may be no apparent decay, the fissures will be somewhat “sticky” to the explorer. Use the fissurotomy bur to perform an excisional biopsy of all the carious and suspect fissure areas (Fig. 4). Explore the fissures for decay with the bur and contour the surrounding enamel to a gentle taper.
2. Complete the tapered preparation to just within the DEJ (Fig. 5). If the caries are shallower, there is no need to go as far as the DEJ. If there is any suspicious dentin or enamel, apply caries detector to the preparation, then wash away after 10 seconds. Any dentin that is stained red should be removed.
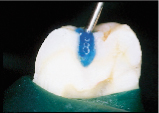
3. Etch the preparation with 37% orthophosphoric acid for 15 seconds (Fig. 6), then rinse thoroughly with air and water. Leave moist for wet-bonding adhesion.
 |
 |
 |
 |
| Figure 4: Fissurotomy bur accessing the fissures. | Figure 5: Final preparation, tapered walls, ending just inside the DEJ (cross-section). | Figure 6: Etching the preparation. |
Figure 7: Application of Excite adhesive. |
4. Apply Excite (Ivoclar North America, Amherst, NY) to the water-moistened preparation (Fig. 7) and allow 15 to 20 seconds for hybridization to occur.
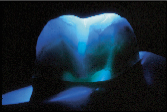
5. Blow off the excess solvent with a one-second blast of air. Light cure for 10 seconds (Fig. 8).
 |
 |
 |
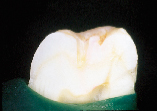
| Figure 8: Light curing the adhesive inside the preparation (note light transmission through enamel). | Figure 9: Injecting the Heliomolar Flow into the preparation. | Figure 10: The cured, finished ultraconservative restoration (note the minimal width of the restoration). |
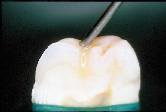
6. Inject the Heliomolar Flow into the preparation (Fig. 9). Light cure for 20 to 40 seconds, depending on the depth of the fissure.
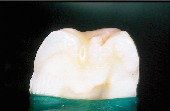
7. Check the occlusion. Reduce and polish the occlusal surface of the composite material as required. Note that in Fig. 10, the ultraconservative width of the restoration is 1/8 to 1/10 the intercuspal distance, as compared to a conventional small amalgam, which is 1/3 to 1/2 the intercuspal distance.
The fissurotomy technique offers an innovative bur design and restorative system that allow both quick treatment and patient comfort, using instruments that are familiar to the dentist and that do not require an investment in new equipment.
Ultraconservative dentistry represents a great step forward for the dentist, the profession, and especially the patient. It involves the early detection and complete elimination of all accessible and non-accessible carious material from the tooth. Untreated caries can be extremely and rapidly destructive. The earliest interception of decay maintains total dental health and increases the likelihood of the restored teeth lasting a lifetime.a
Drs. Freedman, Goldstep and Pakroo are in private practice in Markham, Ontario.
Dr. Seif is in private practice in Caracas, Venezuela.
Reprint requests to: Dr. George Freedman, 675 Cochrane Dr., Suite 508, Markham, ON L3R 0B8
Drs. Freedman and Goldstep provide consultative services to numerous companies.
1. Al-Sehaibany F, White G, Rainey JK. The use of caries detector dye in diagnosis of occlusal carious lesions. J Clin Pediatr Dent 1996; 20:293-8.
2. Wenzel A, Hintze H, Mikkelsen L, Mouyen F. Radiographic detection of occlusal caries in noncavitated teeth. A comparison of conventional film radiographs, digitized film radiographs, and RadioVisioGraphy. Oral Surg Oral Med Oral Pathol; 1991; 72:621-6.
3. Weerheijm KL, Gruythuysen RJ, van Amerongen WE. Prevalence of hidden caries. ASDC J Dent Child 1992; 59:408-12.
4. Ricketts D, Kidd E, Weerheijm K, de Soet H. Hidden caries: What is it? Does it exist? Does it matter? Int Dent J 1997; 47:259-65.
5. Ismail AI. Clinical diagnosis of precavitated carious lesions. Community Dent Oral Epidemiol 1997; 25:13-23.
6. Verdonschot EH, Bronkhorst EM, Burgersdijk RC, Konig KG, Schaeke MJ, Truin GJ. Performance of some diagnostic systems in examinations for small occlusal carious lesions. Caries Res 1992; 26:59-64.
7. Weerheijm KL, de Soet JJ, van Amerongen WE, de Graaff J. Sealing of occlusal hidden caries lesions: an alternative for curative treatment? ASDC J Dent Child 1992; 59:263-8.
8. Handelman SL, Washburn F, Wopperer P. Two-year report of sealant effect on bacteria in dental caries. JADA 1976; 93:967-70.
9. Handelman SL. Effect of sealant placement on occlusal caries progression. Clin Prev Dent 1982; 4:11-6.
10. Mertz-Fairhurst EJ, Smith CD, Williams JE, Sherrer JD, Mackert JR Jr, Richards EE and others. Cariostatic and ultraconservative sealed restorations: six-year results. Quintessence Int 1992; 23:827-38.
11. do Rego MA, de Araujo MA. A 2-year clinical evaluation of fluoride-containing pit and fissure sealants placed with an invasive technique. Quintessence Int 1996; 27:99-103.