
![]()
![]()
Justification raisonnée de la rétention aprčs un traitement d’orthodontie
Marielle Blake, B.Dent.Sc., FDS(Orth.), D.Orth., M.Orth., MRCDC
M. Thérčse Garvey, B.Dent.Sc., M.Sc., FDS, D.Orth., M.Orth
SOMMAIRE
Aprčs un traitement d’orthodontie, une des difficultés majeures de la procédure tout entičre est d’en maintenir les résultats. Les changements qui se produisent normalement pendant la maturation, combinés ŕ ceux qui découlent du traitement orthodontique, compromettent la stabilité ŕ long terme. Dans cet article, on explique pourquoi la rétention est nécessaire et présente un aperçu des appareils couramment utilisés.
Pertinence clinique
La rétention permanente est de plus en plus recommandée comme le seul moyen d’assurer, ŕ long terme, la stabilité des résultats d’un traitement d’orthodontie. Les praticiens dentaires devraient connaître les raisons qui rendent la rétention nécessaire et savoir comment sont conçus les appareils que portent leurs patients.
Mots-clés MeSH: orthodontics; corrective orthodontic retainers; orthodontic wires; tooth movement; malocclusion/pathology; malocclusion/therapy; orthodontic appliances.
© J Can Dent Assoc 1998; 64:640-3
Cet article a fait l'objet d'une révision par des pairs.
[
Introduction | The Need For Retention | Commonly Used Retainers | Positioners | Removable Acrylic Retainers | Essix Thermoplastic Copolyester Retainers | Spring Retainers | Recommendations For Retention Following Orthodontic Treatment | Acknowledgements | References ]
Retention following orthodontic treatment has been defined by Moyers as,“The holding of teeth following orthodontic treatment in the treated position for the period of time necessary for the maintenance of the result.”1 The retention phase is considered by some to be one of the most difficult aspects of the entire orthodontic treatment process. Oppenheim’s statement in 1934 that, “Retention is the most difficult problem in orthodontia; in fact it is the problem,”2 still holds true in many cases today.
The rationale for holding the teeth in their treated position is to:
• allow for reorganization of the gingival and periodontal tissues;
• minimize changes due to growth;
• permit neuromuscular adaptation to the corrected tooth position; and
• maintain teeth in unstable positions (sometimes necessary due to compromise or esthetics).
Before a discussion of changes related to orthodontic treatment, a review of normal maturational dentoalveolar adaptation is warranted. During normal development a moderate increase in arch width is seen until the permanent cuspid erupts.3,4 From this time, a reduction in intercanine width is noted.5-7 The intermolar width remains stable from 13 to 20 years,1,3,4,6,7 and there is a reduction in mandibular arch length with time.3,6-11 An increase in lower incisor crowding occurs during the teenage years, a finding which is more pronounced in females.6,7
Several long-term retention studies evaluating arch stability following different treatment modalities have been carried out. Similar long-term alterations in arch form are reported in most of the treatment groups studied. It is not possible to predict these post-treatment arch changes using variables such as Angles classification, length of retention, patient’s age, gender, pre-treatment overbite, overjet, arch width or arch length.
Following orthodontic treatment, a reduction in arch length and intercanine width is evident. Intermolar width, if expanded during treatment, tends to return toward the pre-treatment value. The reported changes in intercanine and intermolar width are greater in the mandibular arch than the maxillary arch. Although most of the arch changes are seen before age 30, mandibular anterior crowding continues into the fifth decade. As summarized by Little,12 “Treated cases should be viewed as dynamic and constantly changing, at least through the third and fourth decade and perhaps throughout life.”
Most of the treatment modalities studied showed very poor long-term mandibular incisor alignment post retention, with more than one-quarter of all cases showing marked crowding.12-15 Only three treatment modalities showed acceptable long-term results. These were the early mixed dentition treatment without fixed appliance therapy,16 the non-extraction therapy with generalized spaces,17 and the lower incisor extraction cases.18
For these reasons, orthodontists are turning toward permanent retention to ensure stability of post-treatment tooth positions. The biologic aims to be considered when choosing a retainer are:
• maintenance of periodontal support;
• maintenance of optimal oral hygiene; and
• maintenance of functional forces on all the teeth.
Bonded Cuspid To Cuspid Retainers
These fixed retainers are constructed from .0195” or .0175” multistrand stainless steel archwire. An indirect technique is used to adapt the wire passively to a working model. The retainer is attached to the lingual surface of the teeth using floss or a specially constructed jig and is bonded in position using a light-cured composite resin. Care should be taken to clear the occlusion during placement in the maxillary arch. Excess bond on the lingual surfaces and at the gingival margins should be carefully removed, and the area polished giving smooth even surfaces which are easy to clean (Fig. 1).
The inherent flexibility of this multistrand archwire allows for physiologic tooth movement and prevents bond fracture due to occlusal forces. Periodontal ligament stability is also readily achieved using this non-rigid system.19,20 Disadvantages of this mode of retention include possible hygiene difficulties, and localized relapse where there is a partial debond of the retainer. Undetected debonds also carry the risk of decalcification and caries.
While the retainers are in position, the patient should be recalled every six months. Currently, there is much controversy regarding the role of the orthodontist versus that of the referring general practitioner in this long-term maintenance of fixed bonded retainers.
Positioners are elastomeric or rubber removable retainers that are either preformed or custom made. Preformed positioners are available for bicuspid extraction cases and non-extraction cases. Sizes are determined by measuring the mesiodistal dimensions of the six anterior teeth. These preformed positioners cannot compensate for individual variation in the size of the teeth, arch width, arch form or tooth size discrepancies. For these reasons, they should only be used temporarily, if at all.
Custom-made positioners are fabricated on articulated models in which teeth from both arches have been sectioned from the models, realigned and waxed in an ideal configuration. This incorporates minor corrections in tooth position and occlusal relationship. The elastomeric or rubber material is then formed around the teeth and the coronal portion of the gingiva (Fig. 2).
Positioners are worn full time for the first two days, and for four hours daily plus during sleep after that. For the four hours of wear, patients are advised to repeat a cycle of biting and clenching for 20 seconds followed by a rest of 20 seconds. If this routine is followed, the desired tooth movements should have occurred in the first three weeks and the positioner becomes a passive rather than an active appliance.
Disadvantages of this technique include the cost and delay in fabrication of the appliance, the inability to hold rotational and overbite corrections, and the general lack of patient compliance and acceptance.
These include Hawley retainers (Fig. 3), wrap around retainers (Fig. 4) and Barrer retainers (Fig. 5) and are constructed from a wire framework and acrylic baseplate. They can be modified for active tooth movement by activating the labial bow or by incorporating springs. They are routinely worn full time for three to six months, part time for one year to 18 months, followed by continued wear twice a week.
Patients are advised that this pattern should be maintained as an insurance policy against post-treatment changes in the dentition. Disadvantages of these retainers include speech difficulties in the initial period of wear, poor esthetics and a marked dependence on the patient for continued compliance.
Essix Thermoplastic Copolyester Retainers
These clear thin thermoformed appliances (Fig. 6) are gaining in popularity for orthodontic retention.21,22 Advantages include low cost and ease of fabrication together with patient comfort and acceptability. The recommended retention regimen is the same as with removable acrylic retainers. Due to their inherent flexibility, however, they cannot be used to retain cases in which arches have been expanded during orthodontic treatment.
Spring retainers combine the principles of Hawley-type retainers with those of the tooth positioners. A working model is required on which the teeth are aligned. The traditional spring retainer was a sectional appliance using .028” stainless steel contoured to the labial and lingual surfaces of the teeth, incorporating vertical loops passing distal to the canines. Acrylic is added to the wire following the occlusal and gingival contours of the teeth. When inserted, the retainer springs to engage the malpositioned teeth and move these teeth into the alignment established on the working model (Fig. 7).
Due to the potential for dislodging, swallowing or aspirating the appliance, the design has been modified to include acrylic flanges extending lingually to the first molar and incorporates an occlusal rest. The flange joins the lingual clip via .028” stainless steel wire and does not interfere with the spring action. Spring aligners may also be used with interproximal reduction to correct lower mandibular crowding.
Recommendations For Retention Following Orthodontic Treatment
Retainers should be placed as soon as possible following bracket removal. Retainer wires should not be placed across the occlusion through extraction sites, as spaces may reopen. In the presence of periodontal problems, fixed retention rather than removable is preferred, as removable appliances may lead to pathologic pocket formation in the absence of adequate home care.
The term “change” describes the post-retention tooth position better than “relapse.” Change implies that the teeth do not necessarily move back to their former position nor are they stable during the post-retention phase. We should assume that tooth positions will be unstable, rather than stable in the post-treatment phase. For this reason, we should plan to prevent undesirable change.
Patients and parents should be informed of the likelihood of post-treatment changes before treatment is undertaken. Our limitations as professionals and the patients’ role in the maintenance of the result should be discussed. The reasons for permanent retention are summarized in the following statements. “Orthodontic treatment may temporarily alter the course of continuous physiologic change and possibly for a time even reverse them; however, following mechanotherapy and a period of restraint, the developmental maturation process resumes.”23
“Patients face a normal physiologic process of arch constriction and crowding and only by some artificial means can we guarantee success post-treatment.”24
Dr. Blake is a lecturer/consultant in orthodontics, Department of Child Dental Health, Dublin Dental Hospital, Ireland.
Dr. Garvey is a senior lecturer/ consultant in orthodontics, Department of Child Dental Health, Dublin Dental Hospital, Ireland.
Reprint requests to: Dr. Marielle Blake, Department of Child Dental Health, Dublin Dental Hospital, Lincoln Place, Dublin 2, Ireland.
The authors have no declared financial interest in any company manufacturing the types of products mentioned in this article.

Fig 1: Bonded multistrand retainer.
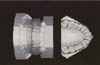
Fig 2: Custom fabricated positioner.

Fig 3: Hawley retainer.

Fig 4: Wrap around retainer.

Fig 5: Barrer retainer.

Fig 6: Essix retainer.

Fig 7: Spring retainer.
References
| 1. | Moyers RE. Handbook of orthodontics for the student and general practitioner. 3rd ed. Chicago, London, Boca Raton: YearBook Publishers Inc.; 1973. |
| 2. | Oppenheim A. Int J Orthod 1934; Vol 6:June. |
| 3. | Moorrees CFA. The dentition of the growing child. Cambridge: Harvard University Press; 1959. |
| 4. | De Kock WH. Dental arch depth and width studies longitudinally 12 years of age to adulthood. Am J Orthod 1972; 62:56-66. |
| 5. | Moorrees CFA, Gron A, Lebret LML, Yen BKJ, Frohlich FJ. Growth studies of the dentition: a review. Am J Orthod 1969; 55:600-16. |
| 6. | Sinclair P, Little R. Maturation of untreated normal occlusions. Am J Orthod Dentofac Orthop 1983; 83:114-23. |
| 7. | Sinclair P, Little R. Dentofacial maturation of untreated normals. Am J Orthod Dentofac Orthop 1985; 88:146-56. |
| 8. | Vego L. A longitudinal study of mandibular arch perimeter. Angle Orthod 1962; 32:187-92. |
| 9. | Fisk RO. Normal mandibular arch changes between the ages of 9 and 16. J Can Dent Assoc 1966; 32:652-8. |
| 10. | Little R. The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod 1975; 68:554-63. |
| 11. | Allred K. Stability and relapse of maxillary anterior alignment. A postretention study of premolar extraction cases treated by traditional edgewise orthodontics [masters thesis]. Seattle (WA): University of Washington, School of Dentistry; 1986. |
| 12. | Little RM, Wallen T, Riedel R. Stability and relapse of mandibular anterior alignment. First premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod 1981; 80:349-65. |
| 13. | Little RM, Riedel RA, Engst D. Serial extraction of first premolars - postretention evaluation of stability and relapse. Angle Orthod 1990; 60:255-62. |
| 14. | McReynolds D, Little R. Mandibular second premolar extractions - postretention evaluation of stability and relapse. Angle Orthod 1991; 61:133-44. |
| 15. | Stein A. A long term evaluation of the mandibular dental arch in non-extraction patients whose arch lengths were held constant or increased in dimensions. University of Washington. Unpublished paper 1974. |
| 16. | Dugoni SA, Lee JS, Varela J, Dugoni A. Early mixed dentition treatment: post-retention evaluation of stability and relapse. Angle Orthod 1995; 65:311-20. |
| 17. | Little RM, Riedel RA. Post-retention evaluation of stability and relapse - mandibular arches with generalised spacing. Am J Orthod 1989; 95:37-41. |
| 18. | Riedel RA, Little RM, Bui DT. Mandibular incisor extraction- post-retention evaluation of stability and relapse. Angle Orthod 1992; 62:103-16. |
| 19. | Artun J. Caries and periodontal reactions associated with long term use of different types of bonded lingual retainers. Am JOrthod 1984; 86:112-8. |
| 20. | Becker A, Goultschin J. The multistrand retainer and splint. Am J Orthod 1984; 85:470-4. |
| 21. | Sheridan JJ, LeDoux W, McMinn R. Essix retainers; Fabrication and supervision for permanent retention. J Clin Orthod 1993; 27:37-45. |
| 22. | Sheridan JJ, LeDoux W, McMinn R. Essix retainers; Essix Technology for the Fabrication of Temporary Anterior Bridges. J Clin Orthod 1994; 28:482-6. |
| 23. | Horrowitz S, Hixon E. Physiologic recovery following orthodontic treatment. Am J Orthod 1969; 55:1-4. |
| 24. | Little RM. Stability and relapse of dental arch alignment. Review Article. Br J Orthod 1990; 17:235-41. |