
![]()
![]()
Le fluorure libķrķ par les matķriaux de restauration esthķtiques : rapport de 12 mois
Y.E.Y. Aboush, BDS, M.Sc., PhD, HD
H. Torabzadeh, DMD, M.Sc.
SOMMAIRE
Historique
Dans cette ķtude, on a calculķ pendant 12 mois la quantitķ de fluorure libķrķ par
trois ciments en rķsine polyalkķonate (ionomĶre de verre) photosensible : un en rķsine
polyalkķonate traditionnelle, un en compomĶre et un en rķsine composite fluorurķe.
Mķthodes
On a plongķ, l’un aprĶs l’autre, cinq disques (7 x 2 mm) de chaque matķriau
dans des parties de 4 mL d’eau dķsionisķe Ó 37░ C et, avant chaque mesure,
rinńait le spķcimen d’essai avec 1 mL d’eau dķsionisķe. Pour les mesures, on
s’est servi d’un microprocesseur numķrique Ionalyser de marque Orion, modĶle
901, et a converti les donnķes obtenues en Ąg/cm 2 . Pendant la pķriode d’essai de
12 mois, on a mesurķ 86 fois la quantitķ de fluorure libķrķ.
Rķsultats
On a dķcouvert que le mode de libķration du fluorure provenant des rķsines
polyalkķonates photosensibles similaire Ó celui de la rķsine polyalkķonate
traditionnelle. Cependant, les rķsines polyalkķonates photosensibles libĶrent beaucoup
plus de fluorure que la rķsine polyalkķonate traditionnelle. La rķsine composite et le
compomĶre libĶrent beaucoup moins de fluorure que toute rķsine polyalkķonate testķe,
la diffķrence entre les deux ķtant nķgligeable.
Conclusion
On a conclu que les rķsines polyalkķonates photosensibles testķes libĶrent plus de
fluorure qu’une rķsine polyalkķonate traditionnelle, un compomĶre ou une rķsine
composite et que, eu ķgard Ó la libķration de fluorure, le compomĶre se comporte plus
ou moins comme la rķsine composite.
Mots clķs MeSH:glass ionomers; composite resins; fluorides/chemistry; materials testing; comparative study.
[ Introduction | Materials and Methods | Results | Discussion | Acknowledgements | References ]
Despite gross microleakage at the silicate restoration-tooth interface, a lower incidence of secondary caries in the restored teeth, as well as in teeth adjacent to these restorations has been reported.1 Such anticariogenic properties of silicate cements were believed to be due to the ability of the material to release fluoride throughout the life of the restoration.2
The pattern and quantity of fluoride released from the conventional glass polyalkenoate (ionomer) cements were reported to be similar to those of silicate cements.2 It has also been shown that conventional glass polyalkenoates provided protection against surface and cavity-wall lesions in the restored teeth.3-6
The preventive effects of fluoride released from silicate and conventional glass polyalkenoate cements have encouraged dental materials manufacturers to incorporate fluoride in a number of other restorative materials such as amalgam,3,7 composite resin 8,9 and a recently introduced material which has been given the generic name “compomer.” These compomer materials are sometimes referred to as “polyacid modified composites” because of their close association with composite resins. The manufacturers of the light-activated (resin-modified) glass polyalkenoates claim that these hybrid materials possess similar fluoride release properties to those of the conventional glass polyalkenoates. However, independent research is required to substantiate these claims.
The aim of this study was to investigate the long-term (12 months) fluoride release from three light-activated restorative glass polyalkenoate cements, a compomer and a fluoridated composite resin in comparison with that from a conventional glass polyalkenoate. Both the 24 hour and cumulative fluoride release were determined.
Five specimens, in the shape of 7mm diameter and 2 mm thick discs, were prepared from each of the six test materials listed in Table I. All materials were dispensed, mixed and light cured, as necessary, in accordance with the manufacturers’ recommendations. One end of a 3cm piece of waxed dental floss was incorporated into each of the disc specimens before the material had set.
| Table I | ||||||||||||||||||||||||||||
| Materials Tested For Fluoride Release Over a 12-Month Period | ||||||||||||||||||||||||||||
|
Immediately after setting of the material, each specimen was suspended inside a plastic bottle containing 4mL of deionized water, except for Fuji Cap II where the specimens spent 15 minutes, from the start of mixing, at 37░C and 100% humidity before being immersed in the deionized water.
The plastic bottles containing the specimens were placed in a water bath at 37░C. After 24 hours, each specimen was removed, rinsed with 1mL deionized water, air-dried using a chip syringe and placed into a fresh 4mL supply of deionized water. The water used for rinsing the specimen was added to the water used for storage to make the test solution.
The fluoride content was determined using an ion-selective electrode system.10 Two mililiters of the test solution were added to 200mL of 0.1mol/L hydrochloric acid (Aristar grade: BDH, Poole, Dorset, UK) to achieve a pHof2. The system was calibrated with fresh standard solutions (1and 10mmol/L) prepared by dilution of 0.1mol/LNaF solution (Orion Research Inc., USA).
The 24-hour regimen of specimen transfer and fluoride content determination was continued for 30 days. On day 31, each specimen was put in 4mL fresh water and was left there for the next 12 days. After that, the specimens were rinsed, dried and placed in fresh water every day for three consecutive days. This regimen was repeated six times over a period of three months. For the following eight months, a similar procedure was followed but with 27-day storage periods instead of 12 days. In total, 86 fluoride determinations were made during the 12-month period of the study.
For periods following the first month, fluoride release was determined on the basis of the amount released during the last of the three consecutive days when the specimens had their storage solution changed.
Results
The fluoride release per 24 hours from the materials, expressed in mg/cm▓, is shown in Fig.1. The fluoride release was high on the first day, fell rapidly over the next day, then gradually decreased to a nearly constant level for all materials except for Tetric where a slight increase was observed before a constant level was reached.
For all materials, the amount of fluoride released was at its highest level during the first 24 hours, followed by a rapid and significant decrease in the next 24 hours, except for Tetric where this decrease was not statistically significant (two-sample t-test at the 0.05 level).
Table II shows the mean amounts of fluoride released from the materials over the last 24 hours of the study period. One-way analysis of variance (ANOVA) indicated a significant difference among the materials (p is less than 0.001). Multiple comparisons between the mean values were then carried out using the Tukey test at the 0.05 level. The results are in Table II.
The cumulative fluoride release data for the 12-month period are shown in Fig. 2 and Table III. ANOVA revealed that there was a significant difference among the materials (p is less than 0.001). The results of the Tukey test, applied to the data, are in Table III.
| Table II | ||||||||||||||
| Means and Standard Deviations Of the Amounts Of Fluoride Released Over the Last 24 Hours Of the 12-Month Test Period | ||||||||||||||
|
| Table III | ||||||||||||||
| Means and Standard Deviations Of the Cumulative Amount Of Fluoride Released During the 12-Month Test Period | ||||||||||||||
|
The techniques used in this study for measuring the fluoride release followed those developed by Tyler and Comer.10 These workers showed that using a constant pH gives the electrodes an increased affinity for fluoride and greater accuracy at lower concentrations than when using TISAB buffer. However, at high concentrations of fluoride (>1mmol/L), both techniques are comparable, but the acid system has the additional advantage of speed, requiring only about two minutes per sample.
All the materials reached constant levels of daily release during the period of this study, though the time to reach this level was different among the test materials. The light-activated glass polyalkenoates reached this constant release sooner than the conventional glass polyalkenoate. This might be due to differences in the setting mechanisms of these materials.
Photac-Fil Aplicap released more fluoride than any other tested material. A similar observation has been reported by other workers.11 The type of glass used in this cement might be the reason for such comparatively high release. However, insufficient information is available regarding the detailed composition of the various cements to enable a meaningful comparison.
All the light-activated glass polyalkenoates released more fluoride than the conventional glass polyalkenoate, the compomer or the composite. This finding is in line with other work where a light-activated glass polyalkenoate liner was found capable of long-term fluoride release and the amount of fluoride released compared favorably with that obtained from two conventional materials.12
It has been reported that the pattern of fluoride release of the light-activated material, Fuji II LC, was virtually the same as its conventional counterpart, FujiCAPII.13 Similar results were obtained in this study. Therefore, it appears that the addition of resins to glass polyalkenoate cements did not affect the fluoride release capability of these materials.
The composite material used in this study, which contained 15% YbF3 released very little fluoride in comparison with the glass polyalkenoate cements. A similar observation was made with another fluoridated composite containing 5% YbF3.14-16 On the other hand, the amount of fluoride released from the composite resin was similar to that released from the compomer. This implies that, with regard to the fluoride release property, the compomer behaves more like a composite than a glass polyalkenoate cement.
There are two mechanisms of fluoride release from dental restorative materials:
1)Dissolution of the material, releasing all its component parts, including fluoride.
2)Diffusion, which can be either the release of fluoride in conjunction with an
appropriate counter ion, typically sodium, or fluoride release via exchange with hydroxyl
groups of the surrounding aqueous environment.
The conventional glass polyalkenoates release via the two mechanisms. The contribution from the dissolution mechanism is greater when the cement is introduced early into water (time is less than 1 hour), as was the case in this study.
The glass polyalkenoate component of the light-activated glass polyalkenoates releases fluoride in a similar manner to that of the conventional material. The contribution from the dissolution mechanism is, however, very little because of the presence of the hydrophobic resins which will repel the water. Composite resins and compomers release fluoride via the diffusion mechanism.
With all the glass polyalkenoate cements tested, solution fluoride concentration was more than 2mg/L (10mg/cm▓) during the first five days, but it dropped below this level soon after. Such relative high initial concentrations in the fluid around a restoration would have a cariostatic effect and also provide a sufficient environment for remineralisation. It was found that 2mg/L fluoride completely inhibited subsurface lesion formation by the inhibition of bacterial acid production and the interaction of fluoride with the enamel mineral during a 10-day study.17
Furthermore, it has been suggested that a high concentration of fluoride would be beneficial in microconservative cavities (e.g. tunnel restorations), where carious dentine and/or enamel remain, due to inadequate access.14 It has also been reported that a fresh glass polyalkenoate cement inhibited the pH fall significantly. However, an artificially aged glass polyalkenoate cement (14 days) was unable to do the same.18 This is presumably because, by this time the rate of fluoride release is much lower (Fig. 1).
An in vitro study showed complete protection against secondary lesion formation in cavity walls and a reduction in the extent of lesion formation adjacent to conventional glass polyalkenoate restorations.4 Also, it was found that in cavities restored with conventional glass polyalkenoates and subjected to a cariogenic medium, the area of demineralisation was some distance away from the cavity wall and the depth of lesion penetration was less with glass polyalkenoate restorations than with composite restorations containing no fluoride.6
In addition, it has been reported that a strong positive correlation was found between the fluoride content of the restorative material and the observed thickness of the surface zone of the outer carious lesion.3 Furthermore, a strong negative correlation was observed between the fluoride content of restorative materials and the extension and penetration of the wall lesions.3 From thesein vitro findings, it appears that the light-activated glass polyalkenoate cements, which were found to release significantly more fluoride than conventional glass polyalkenoates, should have at least the same potential in protecting tooth integrity as that of conventional materials.
However, the fluoride concentration required to obtain a long-term anticariogenic effect, in vivo, has not been established. Furthermore, there is no conclusive evidence to suggest that glass polyalkenoates are significantly better than other materials, in reducing the incidence of secondary caries.19 Mj÷r 20 looked at the reasons for replacement of restorations in general dental practice in Sweden. He reported that: secondary caries was the main reason for the replacement of amalgam, composite and glass polyalkenoate restorations. He found no statistically significant differences in the diagnosis of secondary caries between composite and glass polyalkenoate restorations. Secondary caries was significantly higher for amalgam restorations than for composite and glass polyalkenoate restorations, and half of the glass replaced polyalkenoates were diagnosed as having secondary caries. Similar results have been reported by other workers. 21-23
These findings strongly indicate that the fluoride release from restorative materials is not the sole factor in determining the ability of these materials to prevent secondary caries but, other factors, notably the sealing ability at the margins, play an important role as well.
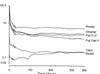
Fig 1: Fluoride release in 24-hour periods.
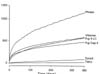
Fig 2: Cumulative fluoride release.
Dr. Y.E.Y. Aboush is a lecturer in restorative dentistry, department of oral and dental sciences, Uni-versity of Bristol, UK. He is also a visiting professor at Dalhousie University, Halifax, Nova Scotia.
Dr. H. Torabzadehis a PhD student at the University of Bristol, UK.
Reprint requests to: Dr. Y.E.Y. Aboush, Department of Oral and Dental Science,
University of Bristol Dental Hospital and School, Lower Maudlin Street, Bristol BS1 2LY, U
K.
| 1. | Council on Dental Materials, Instruments and Equipment. Restorative materials containing fluoride. J Am Dent Assoc1988; 116:762-3. | |
| 2. | Swartz ML, Philips RW, Clark HE. Long-term F release from glass ionomer cements. J Dent Res1984; 63:158-60. | |
| 3. | Hattab FN, Mok NYC, Agnew EC. Artificially formed caries-like lesions around restorative materials. J Am Dent Assoc 1989; 118:193-97 | |
| 4. | Hicks MJ, Flaitz CM, Silverstone LN. Secondary caries formation in vitro around glass ionomer restorations. Quintessence Int1986; 17:527-32. | |
| 5. | Wesenberg G, Hals E. The structure of experimental in vitrolesions around glass-ionomer cement restorations in human teeth. J Oral Rehabil1980; 7:175-84. | |
| 6. | Kidd EAM. Cavity sealing ability of composite and glass-ionomer cement restorations: an assessment in vitro. Br Dent J1978; 144:139-42. | |
| 7. | Jerman AC. Silver amalgam restorative material with stannous fluoride J Am Dent Assoc 1970; 80:787-91. | |
| 8. | Temin SC, Csuros Z. Long-term fluoride release from a composite restorative. DentMater1988; 4:184-6. | |
| 9. | Arends J, Ruben J, Dijkman AG. The effect of fluoride release from a fluoride-containing composite resin on secondary caries: an in vitrostudy. QuintessenceInt1990; 21:671-4. | |
| 10. | Tyler JE, Comer JEA. Novel ion-selective electrode system for the simultaneous determination of fluoride and calcium in acid solution. Analyst 1985; 110:15-8. | |
| 11. | Momoi Y, McCabe JF. Fluoride release from light-activated glass-ionomer restorative cements. Dent Mater1993; 9:151-4. | |
| 12. | Mitra SB. In vitrofluoride release from a light-cured glass-ionomer liner/base. J DentRes1991; 70:75-8. | |
| 13. | Kato S, Tosaki S, Hirota K. Fluoride release from light-cured glass-ionomer cement for restoration. JDentRes 1993; 72, Special edition:221 (Abstract #945). | |
| 14. | Forsten L. Short- and long-term fluoride release from glass-ionomers and other fluoride-containing filling materialsin vitro. ScandJ Dent Res1990; 98:179-185. | |
| 15. | Forsten L. fluoride release and uptake by glass-ionomers. Scand J Dent Res1991; 99:241-5. | |
| 16. | Swift EJ. Fluoride release from two composite resins. QuintessenceInt 1989; 20: 895-7. | |
| 17. | Wahab FK, Shellis P, Elderton RJ. Effects of low fluoride concentrations on formation of caries-like lesions in human enamel in a sequential-transfer bacterial system. ArchOralBiol1993; 38:985-5. | |
| 18. | Seppa L, Torppa-Saarinen E, Luoma H. Effect of different glass-ionomers on the acid production and electrolyte metabolism of Streptococcus mutans ingbritt. CariesRes1992; 26:434-8. | |
| 19. | Erikson RL, Glasspoole EA. Model investigations of caries inhibition by fluoride-releasing dental materials. AdvDentRes1995; 9:315-23. | |
| 20. | Mj÷r IA. The reasons for replacement and the age of failed restorations in general dental practice. ActaOdon-tolScand1997; 55:58-63. | |
| 21. | Kaurich M, Kawakami K, Periz P et al. Clinical comparison: resin and glass ionomer restorations of tooth caries. J Dent Res1989; 68, Special edition:251 (Abstract # 561). | |
| 22. | Levy SM, Jensen ME, Sheth JJ, Doering JV. Clinical evaluation of composite and glass ionomer root caries restorations. J Dent Res1988; 67, Special edition:139 (Abstract #211). | |
| 23. | Randall RC, Wilson NHF. Glass Ionomers: systematic review of a secondary caries treatment effect. J Dent Res1997; 76:1066 (Abstract # 378) |