34
|
Volume1 Issue6
S
upporting
Y
our
P
ractice
etiologyof theproblem, a specific treatment is selected.
Appropriatemanagement of peri-implantitisoften requires
referral toaperiodontist.
Etiology:Bacterial Infection
•
Control theacutebacterial infectionand reduce the
inflammation in the tissues through:
– Mechanical debridement
– Localizedand/or systemicantimicrobial therapy
– Improvedpatient compliancewithoral hygieneuntil a
healthyperi-implant site is established
•
At the re-evaluation, if thepatient does not have a
satisfactory response to thenonsurgical therapy, surgery
shouldbe considered. Assess thepresenceof retained
cement and its subsequent removal (
Figs. 3
and
4
). It is
important to assess for possible cement entrapment, as
newdata shows an increasingnumber of failures from this
etiology.
– Detoxify the implant surfacebyusingmechanical
devices (e.g., highpressureair powder abrasive, laser
decontamination) and/or byapplyingchemotherapeutic
agents (e.g., supersaturatedcitricacidor tetracycline
appliedwithcottonpelletsor abrush).
– Performflapmanagementwitheither (or both) resective
and regenerativeapproaches, dependingon the
morphologyand sizeof thebonedestruction.
– Systemicantibiotics are suggestedpostoperatively.
Etiology:Biomechanical Forces
•
Perform:
– Ananalysisof thefit of theprosthesis
– Averificationof thenumber andpositionof the
implants
– Anocclusal evaluation
Prosthesesdesignchanges, replacingdefective restorative
components, andcorrectingocclusal overload (through improve-
Investigation
•
Verify if iatrogenic factors are involved such as faulty
restoration, impacted foreignmaterial (residual cement),
loose components, etc.
•
Assess if inadequatebiomechanical forces are appliedby
evaluating theocclusion for thepresenceof:
– Parafunction
– Occlusal overload
– Mobilityof the restorativecomponent (removecrown to
assesswhether implant ismobile), fractured restorative
component, fractured implant
•
Look for activeperiodontitis inother sites.
•
Assess thepotential of other bonepathologies.
•
Perform anexploratory surgery.
Diagnosis
Basedon theclinical and radiographicevaluation, adiagnosis
of peri-implantitis isdetermined.
DifferentialDiagnosis
Peri-implantmucositis
Treatment
The long-termgoals are to stop theprogressionof the
diseaseandmaintain the implant site. Dependingon the
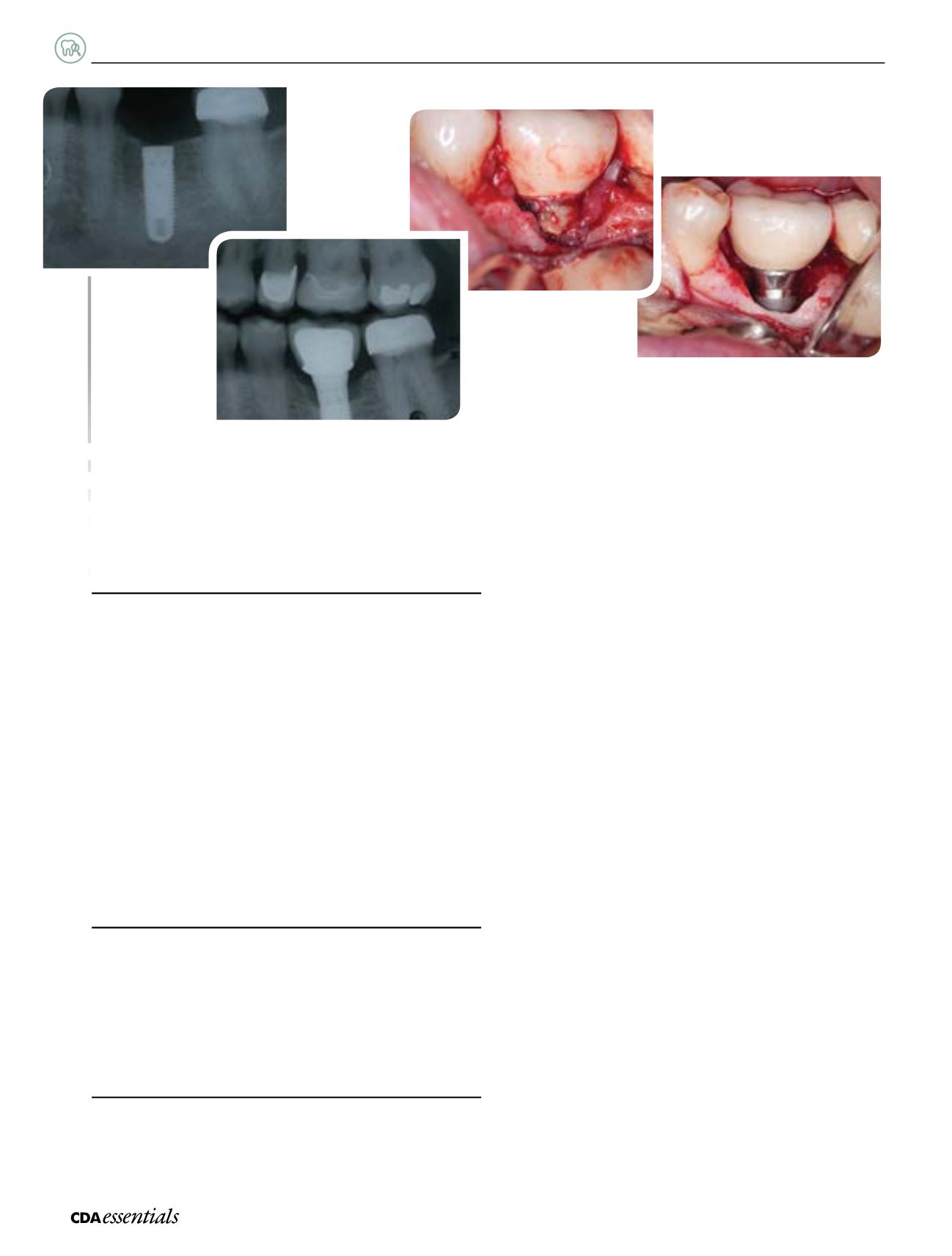
➊
Radiographof implant 36 replacement.
➋
Radiograph showingbone lossof implant 36, at 2-year followup.
➌
Implant 36withcement retained.
➍
Implant 36withcement removed.
➊
❹
➌
➋


