• Laura E. Tam, DDS, M.Sc • Abstract
Accurate diagnosis of the presence or absence of disease is a fundamental
requirement in health care. The diagnosis of non-overt occlusal decay is
challenging and can be highly subjective, and its inherent uncertainties can
lead to widely differing treatment decisions. The purpose of this 2-part paper
is to review current knowledge concerning conventional and new diagnostic
methods for occlusal caries. Part I looked at established methods for diagnosing
occlusal decay. These methods have several limitations, particularly in their
ability to diagnose early carious lesions. Part II examines new and emerging
technologies that are being developed for the diagnosis of occlusal decay.
Electrical conductance measurements and quantitative laser- or light-induced
fluorescence represent significant improvements over conventional diagnostic
methods, especially for in vitro applications and particularly with regard to
sensitivity and reproducibility. Proponents of the DIAGNOdent laser fluorescence
system claim that it evaluates the fluorescence that develops when laser light
is incident on areas of demineralization. This noninvasive device is simple to
use and provides quantitative data. Studies supporting its validity are limited
but do suggest good sensitivity and excellent reproducibility. However, the
DIAGNOdent system requires more scientific scrutiny. Although it offers a high
rate of disease detection, it has little ability to indicate the extent of
decay. In all treatment decisions, clinicians must be aware of the limitations
of the diagnostic methods that have been used. Clinical judgment based on the
patient’s case history, visual cues, review of radiographs and probability of
disease is still the most important aspect of optimum patient care. New
technologies may provide supplemental information, but they cannot yet replace
established methods for the diagnosis of occlusal caries.
MeSH Key Words: dental caries/diagnosis; fluorescence; human
lasers/diagnostic use
© J Can Dent Assoc 2001; 67(8):459-63
• Dorothy McComb, BDS, MScD, FRCD(C) •
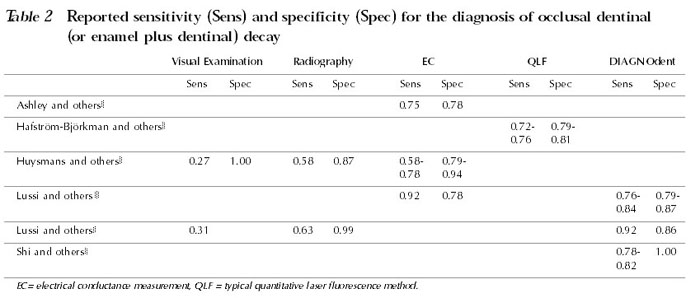
Some of the above-mentioned technologies are suitable only for interproximal or smooth-surface lesions, and others are unsuitable for clinical application. Electrical conductance measurements and laser fluorescence methods (including the DIAGNOdent laser fluorescence device [KaVo, Biberach, Germany]) are 2 distinct technologies with applications in the diagnosis of occlusal caries. The reported sensitivity and specificity for electrical conductance measurements and laser fluorescence methods are presented in Tables 1 and 2.
Electrical Conductance Measurements (EC) The electrical conductivity of a tooth changes with demineralization, even when the surface remains apparently intact. Electrical conductance measurements make use of the increased conductivity of carious enamel in pits and fissures.
The entire occlusal surface is first covered with a conducting medium. Conductivity from the occlusal surface to a ground electrode is then measured with a probe. An increase in conductivity is due to the development of microscopic demineralized cavities within enamel, which are filled with saliva. Two early commercial models of devices for measuring electrical conductance are no longer available, but a new instrument, the Electronic Caries Monitor (Lode Diagnostic, Groningen, The Netherlands), is currently being evaluated. No commercial devices are available in Canada.
Generally high sensitivity and specificity have been reported for EC techniques.4,7,9,10 In one in vivo study, the diagnostic performance of 2 different commercial electronic devices was superior to that of bite-wing radiography, but one device outperformed the other.9 In another study, the in vitro sensitivity of EC was generally superior to that of previously reported visual or radiographic techniques, but its specificity was lower.4 Some concern has been expressed about the level of specificity (below 80%) that has been reported for the Electronic Caries Monitor.4 This translates into a false-positive rate of 20% or a 20% risk of unnecessary operative intervention.
Laser Fluorescence (LF) The LF method measures the fluorescence of the tooth that is induced after light irradiation to discriminate between carious and sound enamel. It is accepted that the induced fluorescence of enamel is lower in areas of reduced mineral content, and that there is a relation between mineral loss and the radiance of the fluorescence.11 The term quantitative laser fluorescence (QLF) has been applied to the research method of measuring induced tooth fluorescence after using laser light generally at or near 488 nm range to quantify tooth demineralization and lesion severity. Several studies in which an argon laser light source (488 nm) was used to examine smooth enamel surfaces have shown a strong correlation between a decrease in fluorescence and the degree of enamel demineralization.12-15 QLF is best suited for longitudinal diagnosis of early lesions of the enamel on accessible smooth surfaces, and many investigations have involved the monitoring of white-spot lesions,12-15 such as those observed in orthodontic patients during treatment and after debracketing.
Fewer studies have assessed QLF for its ability to detect occlusal pit and fissure caries.2,3,8 In in vitro studies of artificial and natural decay of occlusal fissure enamel, QLF had better sensitivity but poorer specificity than visual examination alone or radiographic examination alone.2,3 QLF can be affected to some extent by the wet or dry state of the fissure, by stains in the fissure and by fissure morphology. The use of air-polishing to remove plaque improved diagnosis by QLF.2
Some reports suggest that QLF may be limited to measurement of enamel lesions of at most several hundred micrometres depth.12,13,16 QLF can only discern enamel demineralization and cannot differentiate between decay, hypoplasia or unusual anatomic features. QLF was not designed to discriminate between lesions restricted to the enamel and those extending into the dentin. Furthermore, Banerjee and Boyde17 showed that the fluorescence from dentin was not related to dentin demineralization, so this method is not suitable for measuring dentin demineralization.
DIAGNOdent System A commercial development of LF is the chairside, battery-powered quantitative diode laser fluorescence device (DIAGNOdent). The unit emits light at 655-nm wavelength from a fibre optic bundle directed onto the occlusal surface of a tooth. A second fibre optic bundle receives the reflected fluorescent light beam, and changes caused by demineralization are assigned a numeric value, which is displayed on the monitor. The system is calibrated to a provided standard and to reference (sound) enamel.
The instructions for the DIAGNOdent system specify that the occlusal area to be diagnosed be clean, because plaque, tartar and discolouration may give false values. A laser probe is used to scan over the fissure area in a sweeping motion. Two values are displayed, a current value for the probe position (“moment”) and a maximum value for the whole surface examined (“peak”). The instructions suggest that, in general, numeric data between 5 and 25 indicate initial lesions in the enamel and that values greater than this range indicate early dentinal caries. Advanced dentin caries is said to yield values greater than 35.
Shi and others6 evaluated the DIAGNOdent system in vitro. Surprisingly, the device showed higher diagnostic accuracy in the detection of dentinal caries than enamel caries. The authors suggested that the DIAGNOdent values were dependent on the volume of the caries rather than on the depth of the lesion. With a cut-off of 18 to 22, the sensitivity for diagnosis of dentinal caries in wet teeth was 0.78 to 0.82 (diagnosis confirmed by microradiography of tooth sections). The investigators concluded that overall correlation between DIAGNOdent and microradiography results was moderate but that the device appeared superior to conventional radiography. They reported that the instrument was very sensitive to the presence of stains, deposits and calculus, all of which led to erroneous readings. Similarly, any changes in the physical structure of the enamel, including disturbed tooth development or mineralization, produced erroneous readings. Second (repeated) sets of DIAGNOdent measurements showed better cor relation with the microradiography standard, which was construed as revealing operator learning and skill development. Clinical experience was, therefore, a “fundamental prerequisite” to using the device.
In a similar in vitro study with histological measures as the gold standard, the DIAGNOdent device was compared with EC methods.4 The laser device had sensitivities of 0.76 to 0.84 and specificities of 0.79 to 0.87 whereas the Electronic Caries Monitor had sensitivity of 0.92 and specificity of 0.78 in the measurement of dentinal decay on occlusal surfaces. However, because the DIAGNOdent device had higher specificity than EC and similar sensitivity to EC for the diagnosis of enamel decay, the authors concluded that the DIAGNOdent device had higher diagnostic validity for the detection of the initial carious process. Reproducibility for the DIAGNOdent device was high in this study, but there was also evidence of different degrees of learning for individual dentists, and for 2 of the clinicians reproducibility was poor. The investigators used low cut-off values (10 to 18) for diagnosis and recommended caution in extrapolating their results to the clinical situation. In the end, Lussi and others4 concluded that, because of its rapidity and very high specificity, visual diagnosis remains the method of first choice and they suggested that this type of examination be carried out before any other technique. The DIAGNOdent device could then be used for sites of clinical uncertainty, as a second opinion or diagnostic adjunct.
The results of Shi and others6 and Lussi and others,4 who evaluated the DIAGNOdent device in vitro for the detection of occlusal decay, cannot be directly generalized to clinical practice. The prevalence of caries in those studies was higher than in the typical clinical situation. Furthermore, the extracted posterior teeth were likely cleaner than the true clinical situation because they were stored and/or immersed in a sodium hypochlorite, thymol and/or formalin solution. In clinical practice, therefore, the sensitivity of the DIAGNOdent device will probably be lower.
Lussi and others5 evaluated the DIAGNOdent system in an in vivo study. Air-dried occlusal surfaces of molars and premolars were examined visually (along with bite-wing radiographs if available) and with the DIAGNOdent device. The extent of decay was determined by means of an explorer during operative intervention. A high sensitivity (0.92) was reported for the DIAGNOdent device in detecting occlusal dentinal decay. However, the calculated sensitivity was based on a population of teeth with a very high prevalence of caries, since only teeth that appeared clinically to require operative intervention were assessed for the presence of decay. There was a wide range of readings for enamel caries (approximately 7 to 100), superficial dentinal caries (approximately 7 to 100) and deep dentinal caries (approximately 12 to 100), and the ranges for each overlapped considerably. The DIAGNOdent device was not able to distinguish clearly between deep dentinal caries and more superficial dentinal caries.
Unanswered Questions The DIAGNOdent system is the only LF-related method available commercially for clinical application. However, the available documentation for its use is limited and involves primarily in vitro studies. Whereas the basic research behind the typical QLF technique, which uses lower wavelength light, is relatively plentiful, little documentation exists for the measurement of enamel fluorescence with the red 655-nm diode laser light source used in the DIAGNOdent system.
Many concerns regarding the DIAGNOdent system remain. For example, there is no basic research to show the correlation between DIAGNOdent measurements and the degree of tooth demineralization. The typical QLF methods use a 520-nm high-pass filter to receive the 540-nm autofluorescent light from enamel and to exclude the lower-wavelength light scattered by the teeth. In contrast, the DIAGNOdent system uses a 680-nm filter and detects caries by measuring changes in fluorescence intensity rather than by analyzing spectral differences.18 The DIAGNOdent system, therefore, is fundamentally different from typical QLF methods, and the basic research for the typical QLF technique cannot be extrapolated to the DIAGNOdent device. It is of considerable concern that scientific evidence showing a direct correlation between the numeric DIAGNOdent reading and the severity of disease is lacking. The absence of such evidence precludes the use of the DIAGNOdent device for monitoring the progression of decay.
Also of concern is how the DIAGNOdent readings relate to the presence of dentinal decay and the need for operative intervention. As stated previously, typical QLF results show a strong correlation with the degree of enamel demineralization only but no correlation with the degree of dentinal decay. Furthermore, correlation with the degree of enamel demineralization is limited in depth.12,13,16 For the DIAGNOdent device, it has been postulated that the diode laser light does not reach deeper dentinal layers,5 which would explain the reported inability of the device to distinguish between superficial and dentinal decay in vivo.
Yet other questions relate to the optimal technique for clinical use of the DIAGNOdent device. At this time, in light of the unanswered questions and given the overall reduction in the prevalence of caries in the population, the clinical value of the device requires further investigation.
Conclusions The development of reliable, accurate quantitative methods to diagnose and monitor early carious lesions is critical. EC and LF demonstrate significant improvements over established diagnostic methods, especially for in vitro applications and particularly with regard to sensitivity and reproducibility. Because of their quantitative nature and high reproducibility, these 2 methods can be used to monitor the progression of a suspected carious lesion and for patient education and motivation. In individual cases, they might also contribute to the decision-making process concerning appropriate preventive and operative strategies in caries management. However, one-time measurements made with EC and LF cannot discriminate between active and inactive lesions, which is also the case with other diagnostic methods. The DIAGNOdent device, a commercial variant of LF technology, is noninvasive and simple to use and provides quantitative measurements. However, more scientific scrutiny is required before it can be recommended for the definitive diagnosis of occlusal decay requiring operative intervention.
No current diagnostic method fulfils all the criteria for optimal caries management. Verdonschot and others19 conducted a meta-analysis on various diagnostic tests. They determined a Dz value, which they considered representative of the probability above chance that the output from a diagnostic test would be correct (true negative or true positive). For diagnosis of occlusal caries, the EC methods demonstrated the highest Dz value relative to visual and radiographic methods; the Dz of QLF was not reported in that paper. However, true QLF correlated best with histological lesion depth or mineral loss of smooth-surface enamel caries. For occlusal surfaces, visual inspection had the highest correlation with histological observations of demineralization.
Incorrect diagnoses result in incorrect treatment decisions. In the current age of lower overall prevalence of decay and slow disease progression, the potential risk of unnecessary restorations is greater than the risk of missing early decay. The potential risk of missing early decay is also lower in patients who return regularly for recall dental examinations. In all treatment decisions, clinicians must be aware of the limitations of the diagnostic methods that have been used. Knowledgeable clinical judgment based on the patient’s case history, visual cues, review of radiographs and probability of disease is a necessity for the provision of optimum care. New technologies may provide supplemental information, but they cannot yet replace established methods for the diagnosis of occlusal caries.
Dr. Tam is associate professor of restorative dentistry, faculty of dentistry, University of Toronto.
Dr. McComb is professor and head of restorative dentistry, faculty of dentistry, University of Toronto.
Correspondence to: Dr. Laura E. Tam, Restorative Dentistry, Faculty of Dentistry, University of Toronto, 124 Edward St., Toronto, ON M5G 1G6. E-mail: laura.tam@utoronto.ca.
The authors have no declared financial interest in any company manufacturing the types of products mentioned in this article.
References 1. Angmar-Mĺnsson B, ten Bosch JJ. Advances in methods for diagnosing coronal caries — a review. Adv Dent Res 1993; 7(2):70-9.
2. Ferreira Zandoná AG, Analoui M, Schemehorn BR, Eckert GJ, Stookey GK. Laser fluorescence detection of demineralization in artificial occlusal fissures. Caries Res 1998; 32(1):31-40.
3. Ferreira Zandoná AG, Analoui M, Beiswanger BB, Isaacs RL, Kafrawy AH, Eckert GJ, Stookey GK. An in vitro comparison between laser fluorescence and visual examination for detection of demineralization in occlusal pits and fissures. Caries Res 1998; 32(3):210-8.
4. Lussi A, Imwinkelried S, Pitts N, Longbottom C, Reich E. Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res 1999; 33(4):261-6.
5. Lussi A, Megert B, Longbottom C, Reich E, Francescut P. Clinical performance of a laser fluorescence device for detection of occlusal caries lesions. Eur J Oral Sci 2001 ; 109(1):14-9.
6. Shi XQ, Welander U, Angmar-Mĺnsson B. Occlusal caries detection with KaVo DIAGNOdent and radiography: an in vitro comparison. Caries Res 2000; 34(2):151-8.
7. Ashley PF, Ellwood RP, Worthington HV, Davies RM. Predicting occlusal caries using the electronic caries monitor. Caries Res 2000; 34(2):201-3.
8. Hafström-Björkman U, Sundström F, Angmar-Mĺnsson B. Initial caries diagnosis in rat molars, using laser fluorescence. Acta Odontol Scand 1991; 49(1):27-33.
9. Huysmans MC, Longbottom C, Pitts N. Electrical methods in occlusal caries diagnosis: an in vitro comparison with visual inspection and bite-wing radiography. Caries Res 1998; 32(5):324-9.
10. Pine CM, ten Bosch JJ. Dynamics of and diagnostic methods for detecting small carious lesions. Caries Res 1996; 30(6):381-8.
11. van der Veen MH, de Josselin de Jong E. Application of quantitative light-induced fluorescence for assessing early caries lesions. Monogr Oral Sci 2000; 17:144-62.
12. al-Khateeb S, ten Cate JM, Angmar-Mĺnsson B, de Josselin de Jong E, Sundström, G., Exterkate RA, Oliveby A. Quantification of formation and remineralization of artificial enamel lesions with a new portable fluorescence device. Adv Dent Res 1997; 11(4):502-6.
13. Emami A, al-Khateeb S, de Josselin de Jong E, Sundström F, Trollsĺs K, Angmar-Mĺnsson B. Mineral loss in incipient caries lesions quantified with laser fluorescence and longitudinal microradiography. A methodologic study. Acta Odontol Scand 1996; 54(1):8-13.
14. Hall AF, DeSchepper E, Ando M, Stookey GK. In vitro studies of laser fluorescence for detection and quantification of mineral loss from dental caries. Adv Dent Res 1997; 11(4):507-14.
15. Lagerweij MD, van der Veen MH, Ando M, Lukantsova L, Stookey G. The validity and repeatability of three light-induced fluorescence systems: an in vitro study. Caries Res 1999; 33(3):220-6.
16. Hafstrom-Bjorkman U, Sundström F, de Josselin de Jong E, Oliveby A, Angmar-Mĺnsson B. Comparison of laser fluorescence and longitudinal microradiography for quantitative assessment of in vitro enamel caries. Caries Res 1992; 26(4):241-7.
17. Banerjee A, Boyde A. Autofluorescence and mineral content of carious dentine: scanning optical and backscattered electron microscopic studies. Caries Res 1998; 32(3):219-26.
18. Hibst R, Gall R. Development of a diode laser-based fluorescence caries detector. Caries Res 1998; 32(Abstr 80):294.
19. Verdonschot EH, Angmar-Mĺnsson B, ten Bosch JJ, Deery CH, Huysmans MC, Pitts NB, Waller E. Developments in caries diagnosis and their relationship to treatment decisions and quality of care. ORCA Saturday Afternoon Symposium 1997. Caries Res 1999; 33(1):32-40.
{kind=link}
{kind=link}