• Susan E. Sutherland, DDS
• Abstract
There is a growing interest in clinical practice guidelines (CPGs)
for all health care providers. As discussed in the first paper of this 2-part
series, there are many misperceptions about guidelines and their potential risks
and benefits. The dental profession in Canada, cognizant of both the importance
and the challenges of developing sound, credible and relevant guidelines for
dentists, has created a unique, autonomous collaboration of multiple
stakeholders, the Canadian Collaboration on CPGs in Dentistry (CCCD). This paper
discusses the history, structure and processes of the CCCD and introduces the
first guideline under development by and for Canadian dentists.
MeSH Key Words: Canada; dentistry; evidence-based medicine; practice
guidelines
© J Can Dent Assoc 2001; 67(8):448-52
Debora C. Matthews, DDS, Dip. Perio., M.Sc. •
• Peter Fendrich, BA, DDS •
There is worldwide interest in the development of CPGs in all areas of health care. Many groups, such as the U.S. Agency for Healthcare Research and Quality, the National Institutes of Health and the Canadian Medical Association, are involved in the development of practice guidelines for the medical profession. However, there are few organizations involved with the development of dental practice guidelines. The Canadian Collaboration on Clinical Practice Guidelines in Dentistry (CCCD) is the national, autonomous body responsible for the creation of evidence-based guidelines for dentistry in Canada. The CCCD is unique in that it is a self-directing organization composed of multiple stakeholders whose mandate is to involve practising dentists in the entire process of creating guidelines for Canadian dentists.
The CCCD was conceived and built by a diverse group of Canadian dentists, cognizant of the barriers, risks, challenges and, above all, potential benefits2,3 of the development of evidence-based CPGs. The organizational structure of the CCCD, as well as the guiding principles and methodological protocol for producing these guidelines, has been laid out in a living document — the CCCD Resource Manual.4 History of the CCCD The CCCD had its conceptual beginnings at a workshop sponsored by the Canadian Dental Association (CDA) in 1997. The participants at the CDA national workshop included delegates from the Canadian faculties of dentistry, the provincial dental associations, specialist groups, provincial dental regulatory authorities (DRAs) and invited guests who had expertise and first-hand experience in the development of practice guidelines. As a result of that workshop, CDA’s ad hoc committee on clinical practice guidelines obtained a mandate from the CDA board of governors to develop a national strategy for CPG development and implementation in dentistry. CDA would assume the role of coordinating and facilitating a national, collaborative approach to CPG development that would be inclusive of all interested stakeholders. In an environment that has health care under ever-increasing scrutiny by various outside interest groups, including governments, it was felt that it was essential for the dental profession to play a lead role in defining high-quality, evidence-based dental care.
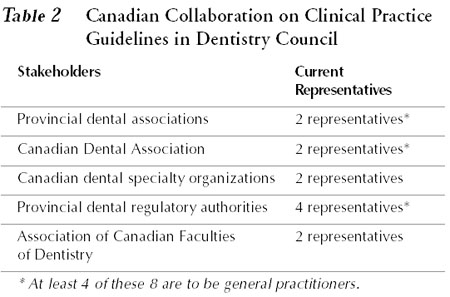
The inaugural meeting of the CCCD was held in Halifax in October 1999 and was attended by representatives of the Canadian and provincial dental associations, the DRAs, the national dental specialty organizations and the Association of Canadian Faculties of Dentistry. At that meeting, concerns were raised regarding a number of issues, including representation and involvement of all relevant stakeholders; funding and human resources; methodology; communication and information management; open, transparent processes; and autonomy of the CCCD. In spite of these concerns, key decisions were made regarding the purpose, duties, representation, overall structure and guiding principles of the CCCD.
A second meeting of the CCCD, held in Toronto in October 2000, led to the creation of a draft constitution, a structured protocol for generating guidelines and the formation of the first working group, tasked to produce the first CPG. The topic selected was “the emergency management of acute apical periodontitis in the permanent dentition.”
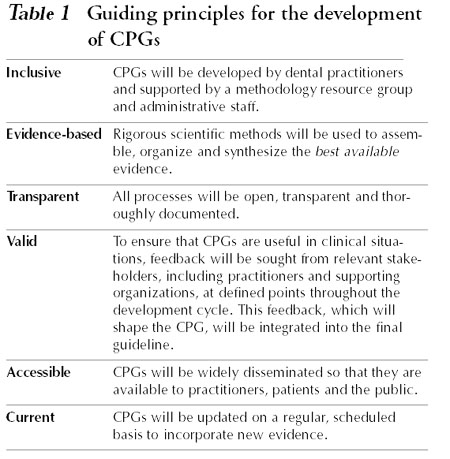
Guiding Principles for the Development of CPGs Principles were established to guide the methodology and processes by which evidence-based CPGs will be developed. These are outlined in Table 1.
Organizational Structure of the CCCD
CCCD Council
The council is responsible for formulating policy with respect to the guideline process, for selecting and prioritizing topic areas in consultation with the profession, and for overseeing the development and dissemination of guidelines.
Clinical Advisory Group The clinical advisory group (CAG) is a multidisciplinary team of volunteer dentists who have a particular interest or expertise in the content area of the guideline topic under development. The CAG is chaired by a person knowledgeable about the methods of guideline development. The group may consist of 2-3 specialists (no more than one of whom should be a full-time academic) and 4-5 general dentists (no more than one of whom should be a full-time academic). This group will not be required to have expertise in the methodology of systematic reviews; it will be made up of practising dentists who have been recommended to the CCCD by their provincial dental associations, specialty organizations or DRAs. The responsibilities of the CAG will be to coordinate the development and production of an individual guideline.
Methodology Resource Group The methodology resource group (MRG) consists of individuals with expertise and methodological skills in the retrieval and evaluation of scientific evidence, or with training and experience in clinical epidemiology or a related discipline. This group will include one or more salaried research assistants, who will assist with the systematic reviews and in the formatting and editing of reports. The group will be chaired by a person knowledgeable about the methodology of systematic reviews. The MRG has 3 primary functions. The first is to provide the methodological support needed by the CAG, enabling the clinicians of the CAG to use sound methodology in the guideline process. The second is to oversee and advise the research assistant(s) who will carry out the technical systematic review and draft evidence-based recommendations, guidelines and reports. Finally, the MRG will provide educational opportunities in methodology for interested participating practitioners and others, at the discretion of the council.
CPG Coordinator The CPG coordinator is a paid administrator who will assume a variety of administrative functions and will report to the CCCD council. Once the process of CPG development is underway, it is anticipated that up to a dozen guidelines will be at some stage of development at any given time. The primary responsibilities of the coordinator will be to liaise with both the CAG and MRG through the respective chairs; to assist each CAG chair with the development of the budget and timeline for that CPG; to oversee each CPG, ensuring that resources are used efficiently and that targeted timelines are met; to aid in the preparation and dissemination of reports; and to schedule and organize the updating activities for each CPG.
Steps in the CPG Process
Identifying the Need for a CPG
The topic or question for a CPG may come to the CCCD from a number of sources, including Canadian dentists, provincial regulatory authorities, dental educators, dental researchers or members of the general public. Topics may be solicited by the CCCD, or submitted by stake holders to the CCCD.
Topics will be prioritized and selected by the CCCD council, in consultation with stakeholder groups. The following criteria7 will be considered in the decision-making process:
Planning Stage Once a topic has been selected, the CCCD council will appoint the chair of the CAG and of the MRG. A literature review will be conducted to identify and evaluate any existing CPGs. Budget and timelines will be determined and the CAG assembled.
Developing the CPG The formation of evidence-based guidelines contains many steps7-10 that incorporate the best available external evidence from clinical research with clinical expertise. The foundation of the approach is the systematic literature review. The following outlines the protocol adopted by the CCCD.
Framing the Clinical Question The CAG will frame the problem by developing a question that focuses on the target population, the exposure or intervention and its comparison, and the specific outcomes of interest.
Conducting a Systematic Review of the Evidence At the direction of the CAG a systematic review of the literature, following a structured protocol, will be done by the research assistant, with methodological support provided by the MRG.
Validating the CPG
Guideline-in-Progress
A final draft of this report, along with a structured questionnaire, will be sent to a representative sample of practising Canadian dentists from a database of potential reviewers for whom the guideline may be relevant. Their input will be sought regarding the quality and completeness of the literature search, the interpretation of the evidence, and the importance, usefulness and implications of the draft recommendations for practice. The information from this first external review will be used to modify the clinical recommendations as necessary.
The modified guideline-in-progress (now a draft CPG) will be sent for comment to the CCCD council and for a second external review to all interested stakeholders, including the national and provincial dental associations, dental specialty organizations, the Association of Canadian Faculties of Dentistry and the Canadian DRAs. The draft CPG will also be sent to other relevant stakeholder groups whose opinion or “buy-in” to the guideline may be important.
CPG Document Following the second external review, the CPG will be sent to the CCCD council for final approval, then edited and formatted for publication. The format of the CPG will include a structured abstract; a statement of the question and the rationale for the choice of topic; a comprehensive methods section; results of the literature search and of relevant outcomes; an interpretative summary; a description of the CAG consensus process; draft recommendations; and the methods, results and modifications generated by the practitioner feedback survey and other external reviews. The subsequent publication of the CPG in the peer-reviewed dental literature will constitute a third external review.
Disseminating the CPG The final CPG will be disseminated widely following a predefined dissemination plan, which is currently being developed. This will likely include a variety of methods11 such as paper publication in the peer-reviewed dental literature, electronic publication on a Web site (full version for practitioners and patient synopsis for consumers), and “academic detailing,” whereby respected peers will present the guideline to colleagues at study clubs and local dental society meetings.
On a pre-defined schedule, the systematic review for each CPG will be updated and new evidence evaluated. If indicated by the presence of new strong evidence, the CPG will re-enter the guideline cycle.
What if the Evidence Is Weak or Lacking? For some clinical topics, the conclusions of the systematic review may highlight very weak or uncertain evidence. The members of the CAG may decide that there is insufficient evidence on which to make clinical recommendations from which a guideline could be developed. The resulting report will then be an evidence summary, which is intended to provide information on the available evidence in a comprehensive, organized manner. The format will include the components described for the CPG document, but will exclude draft recommendations. It may also include optional sections such as:
An evidence summary, like a CPG, will be updated on a regular basis. However, if additional information, found through the updated systematic review, indicates that there is sufficient new evidence to warrant clinical recommendations, a guideline-in-progress will be drafted, which will enter the CPG cycle as outlined previously.
Conclusion We have presented the organizational structure and the methodological protocol adopted by the CCCD for the creation of CPGs for the dental profession in Canada. It is anticipated that guidelines will be produced that are relevant, credible and useful. At the time of this writing, the first guideline on the topic of emergency management of acute apical periodontitis in the permanent dentition is in the beginning stages of development. Completion is expected to take 12 to 18 months. We look forward to reporting the results of this first endeavour to the dental profession at that time.
Dr. Diane Legault
Dr. Dorothy McComb
Dr. Evelyn McNee
Mr. Don Pamenter
Dr. Trey Petty
Dr. Euan Swan
Members of the first council of the CCCD
Dr. Peter Fendrich (chair), Canadian Dental Association
Dr. William Abbott, Canadian Association of Oral and Maxillofacial Surgeons
Dr. Paul Cameron, Nova Scotia Dental Association
Dr. Hugh Campbell, Alberta Dental Association
Dr. Kevin Doyle, College of Dental Surgeons of British Columbia
Dr. Ken Glover, Canadian Association of Orthodontists
Dr. Jacques Laforce, Ordre of Dentists of Quebec
Dr. Lex MacNeil, University of British Columbia
Dr. Don McFarlane, Royal College of Dental Surgeons of Ontario
Dr. Debora Matthews, Dalhousie University
Dr. Susan Sutherland, Ontario Dental Association Dr. Euan Swan, Canadian Dental Association
CDA staff support
Ms. Anne Bauer
Mr. Brian Henderson
Dr. Benoit Soucy
Acknowledgments: The CCCD has become a reality as a result of the efforts of many individuals. We thank the supporting organizations and all participants at early workshops for providing the inspiration and framework for the collaboration. In particular, we thank CDA for its ongoing assistance and encouragement. The CCCD also gratefully acknowledges Drs. Melissa Brouwers and George Browman and Ms. Anna Gagliardi from the Program in Evidence-Based Care, Cancer Care Ontario, for generous sharing of resource materials, as well as their support and practical advice.
Dr. Sutherland is a full-time active staff member of the department of dentistry at the Sunnybrook and Women’s College Health Sciences Centre, University of Toronto in Toronto. She is the vice-chair of the Canadian Collaboration on CPGs in Dentistry.
Dr. Matthews is head of the division of periodontics in the faculty of dentistry, Dalhousie University, and a member of the Canadian Collaboration on CPGs in Dentistry.
Dr. Fendrich is a general practitioner in London, Ontario, and an adjunct professor in the department of oral medicine in the faculty of medicine and dentistry, University of Western Ontario. He is chair of the Canadian Collaboration on CPGs in Dentistry.
Correspondence to: Dr. Susan E. Sutherland, Department of Dentistry, Sunnybrook and Women’s College Health Sciences Centre, 2075 Bayview Ave., Toronto, ON M4N 3M5. E-mail: susan.sutherland@swchsc.on.ca
The views expressed are those of the authors and do not necessarily reflect the opinions or official policies of the Canadian Dental Association.
References 1. Field M, Lohr K. Clinical practice guidelines: directions for a new program. Institute of Medicine. Washington (DC): National Academy Press; 1990.
2. Woolf SH. Practice guidelines: a new reality in medicine. III. Impact on patient care. Arch Intern Med 1993; 153(23):2646-55.
3. Woolf SH, Grol R, Hutchinson A, Eccles M, Grimshaw J. Clinical guidelines: potential benefits, limitations, and harms of clinical guidelines. BMJ 1999; 318(7182):527-30.
4. Sutherland S, Matthews D. Canadian Collaboration on CPGs in Dentistry. Resource Manual. Ottawa, Canada; 2001.
5. Jutras D. Clinical practice guidelines as legal norms. CMAJ 1993; 148(6):905-8.
6. Caulfield T. What impact do CPGs have on the practice environment and on care? A legal perspective. In: Ushjer S, editor. Scripting a future for clinical practice guidelines; 1999. Toronto, Canada: Health Policy Forum; 1999.
7. Hayward RS, Laupacis A. Initiating, conducting and maintaining guidelines development programs. CMAJ 1993; 148(4):507-12.
8. Woolf SH, Battista RN, Anderson GM, Logan AG, Wang E. Assessing the clinical effectiveness of preventive maneuvers: analytic principles and systematic methods in reviewing evidence and developing clinical practice recommendations. A report by the Canadian Task Force on the Periodic Health Examination. J Clin Epidemiol 1990; 43(9):891-905.
9. Browman GP, Levine MN, Mohide EA, Hayward RS, Pritchard KI, Gafni A, and others. The practice guidelines development cycle: a conceptual tool for practice guidelines development and implementation. J Clin Oncol 1995; 13(2):502-12.
10. Cluzeau FA, Littlejohns P, Grimshaw JM, Feder G, Moran SE. Development and application of a generic methodology to assess the quality of clinical guidelines. Int J Qual Health Care 1999; 11(1):21-8.
11. Randall G, Taylor DW. Clinical practice guidelines: the need for improved implementation strategies. Healthc Manage Forum 2000; 13(1):36-42.
THE CCCD NEEDS YOU!!
The Canadian Collaboration on
Clinical Practice Guidelines in Dentistry (CCCD) is the national, autonomous
body responsible for the creation of evidence-based guidelines for dentistry in
Canada. Clinical practice guidelines (CPGs) summarize the best available
research evidence on a particular topic to provide guidance for dentists and
patients. One of the key principles of the CCCD is that CPGs in Canada will be
developed BY dentists, FOR dentists.
Who can be involved?
All dentists practising in Canada are eligible
to be entered into the database of potential reviewers. An academic, research or
specialty background is NOT necessary.
What does a reviewer have to do?
For each guideline, a random sample of
reviewers will be drawn from the database. Each reviewer will be sent a
preliminary draft of the guideline under development and a structured
questionnaire. Feedback will be sought regarding the methods used to create the
guideline and the importance, usefulness and implications of the draft
recommendations for practice. The information from this feedback will be used to
modify the clinical recommendations as necessary.
What about confidentiality?
Your privacy in registering for the database
will be assured. The information you provide will ONLY be used to contact
volunteers for this initiative. Confidentiality of the reviewers will be
maintained. No individuals will be identified in any report or publication of
the CCCD.
How do I register for the CCCD database?
Please contact: Monica Farrag, CCCD Research
Assistant, c/o Department of Dental Clinical Sciences, Dalhousie University,
5981 University Avenue, Halifax NS B3H 3J5 Fax: (902) 494-1662; e-mail: mfarrag@is2.dal.ca
For online registration, please visit our Web site at www.cccd.ca.
{kind=link}
{kind=link}