• H. Sharon Campbell, PhD •
Abstract
MeSH Key Words: counselling; dentists; tobacco use cessation
© J Can Dent Assoc 2001; 67:141-4
• Elizabeth H. Simpson, M.Sc. •
• Trey L. Petty,
BA,
B.Sc., DDS •
• Penny A. Jennett, PhD •
Most smokers need encouragement and motivation to quit. The dental office can provide counselling in a new and highly relevant context. The oral effects of tobacco appear much earlier than the systemic effects and are visibly reversed when smoking is stopped. Use of the intraoral camera allows dentists to actually show this change to patients, which gives them an advantage over other health professionals. In addition, men and teenagers regularly present for dental visits whereas they are less likely to see a physician. Thus dental care providers can reach a group of smokers who may not receive other professional advice. These are important reasons for the dental profession to move quickly to incorporate TCS into routine practice.
However, there has been a reluctance to do so. Adding or expanding TCS is very much like adding other new services. It takes time before the new service becomes part of a comfortable routine. And while the dentist must agree to add TCS to the practice, the whole staff must be involved in the decision, as it is often the hygienist or assistant who will provide the actual TCS. Deciding on the range of services to offer is a key factor. At a minimum, displaying self-help cessation materials in the reception area will provide interested quitters with resources they may not access otherwise. At the other end of the spectrum, it is possible to envisage establishing a full-scale cessation clinic. In between, there is a level of service that fits with the practice pattern and patient needs of every office.
A Canadian First In 1996, 54 Alberta dentists agreed to participate in a 2-year randomized controlled trial designed to test an educational program aimed at improving TCS offered by dental offices.11-13 Offices were randomized to an intervention or a control group. The intervention group received an office cessation manual, patient education materials, performance feedback and participated in teleconferences with colleagues. These interactions proved essential — the opportunity to exchange with others, to share concerns and strategies with colleagues, and to learn about patient response to TCS were critical in the adoption of a new practice.
Baseline data collected from office staff and patients showed that less than half the dental offices routinely advised patients to quit smoking. And while the intervention group almost doubled the proportion of smokers advised to quit by the end of the study (15.6% to 27.0%) compared to the control group (12.2% to 15.1%, p = 0.02), there still remains a large unexploited opportunity to help patients quit tobacco use and protect their oral health.
Approaching Tobacco Cessation Study participants identified the following barriers to the inclusion of TCS: patient resistance and alienation; the time required to provide the services; ineffectiveness in getting patients to quit; and lack of both patient education materials and referral resources. All these concerns can be easily addressed and need not stand in the way of providing a much needed service.
Concerns about patient resistance and alienation are largely in the minds of the dental professionals. In the Alberta study, 61.5% of dentists thought patients did not want to receive advice about quitting from the dental office, yet almost the same percentage (59.0%) of tobacco users felt their dentist ought to provide such advice. Another 13.8% of users were unsure about receiving cessation advice from their dentist, but not negative.13 It is therefore dentists’ perception more than anything that prevents the profession from moving forward in providing TCS.
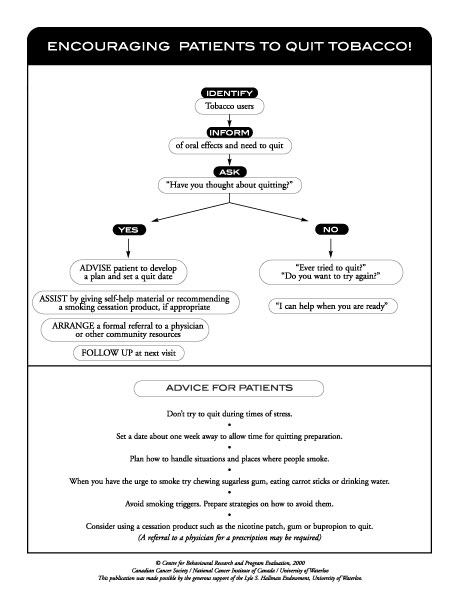
The time factor is a realistic concern, but streamlining TCS to meet both patient needs and the requirements of a busy practice is possible. The key is to incorporate TCS into routine patient care. All smokers should be aware of the oral problems associated with tobacco use and should be advised to quit. To date, lay literature has ignored the oral effects of cigarette smoking and patients may not be aware of this association. Just as poor hygiene and nutrition are discussed in relation to perio dontal disease, so too should tobacco use. It should become part of the list of causal factors that are routinely discussed. Once smokers are identified, a simple question about their interest in quitting allows one to triage them to an appropriate level of intervention. Prochaska14 classifies smokers into precontemplators (those not interested in quitting), contemplators (those interested but not ready), and active quitters (those making a quit attempt). Although there has been some debate recently about the scientific strength of this model,15 it provides a useful approach to streamlining TCS. For smokers not interested in quitting, a simple offer to assist when they are ready takes less than 15 seconds, is not offensive, and reminds them that help is available when needed. For patients interested in quitting, the provider can offer self-help resources, refer them to their physician or community cessation programs, or spend a minute or 2 discussing plans for quitting. For motivated quitters, helping to set a realistic quit date is often the impetus needed to make a serious attempt. For smokers actively quitting, providing encouragement and discussing relapses as lessons learned takes only a few minutes. All can be done as part of the chair-side consultation without adding significant time to the appointment (Table 1).
One of the barriers to incorporating TCS into dental practice has been an unrealistic focus on quit rates as the goal. In reality very few smokers actually quit as the result of a single professional intervention. Smokers make many attempts before they are successful. It is consistent, repeated advice and assistance that make the difference. Thus the role of the dental team becomes one of encouraging, prompting and helping patients plan for a quit attempt. With this in mind, concerns about provider ineffectiveness and smokers’ inability to quit need not be barriers to providing TCS. The goal of the dental practice becomes one of informing smokers about the oral health effects of tobacco use, advising them to quit and providing assistance as needed.
The final major barrier identified by our study participants was lack of both patient education materials and referral resources. Most dental offices work in the realm of private practice and may be unaware of community resources that can be accessed by smokers. Three of the major health charities (Canadian Lung Association, Heart and Stroke Foundation of Canada, Canadian Cancer Society) provide self-help cessation materials. Smokers can be referred to these organizations or their materials ordered and displayed in the office reception area. Displaying self-help materials not only identifies a practice as supporting cessation but encourages patients to approach staff about quitting. Many patients would do so if they knew help was available. The Canadian Cancer Society also operates a toll-free cancer information service (1-888-939-3333) throughout Canada. Assistance, self-help materials and referral to other resources are provided by trained information specialists. The local public health unit will be knowledgeable of other programs and resources within the community. A patient’s family doctor is also an important player in cessation efforts and can be a useful ally in providing TCS. Helping patients quit is not something the dental office has to do alone — there are many community resources available and a simple phone call can link the dental office to a network of tobacco resources.
Keys to Success The Alberta study revealed 5 keys to success:
1. teamwork — offices where all staff were involved in providing TCS were more successful;
2. an office champion with overall responsibility for the program makes a positive difference;
3. simple, consistent service over time is more successful than intermittent, more intense interventions;
4. the sharing of experiences with peers and colleagues encourages adoption;
5. a connection to community resources provides options for appropriate referrals.
The time has come for the dental profession to make tobacco cessation a priority. The evidence linking cigarette smoking and periodontal disease is strong and requires that smokers receive proper patient care, just as they would for any other threat to their oral health. The reluctance of the dental profession to address tobacco use stems in large part from the concerns discussed above — all of which can be addressed. Each individual dentist must make the decision to offer some level of service, whether it be simply providing patient education materials or helping patients plan their next quit attempt. Dental offices may prefer to start by offering patient resources, and as staff comfort and confidence increase, add components of a comprehensive program. The day will come when all patients who use tobacco can access professional assistance from their dental office. This will not occur overnight, but like any change, happens one person at a time. The time to start is now.
The Profession’s Responsibility In addition to individual commitment on the part of dentists, the profession itself can help create an environment that enhances the rate of adoption. Rogers’ classic work on innovation diffusion has shown that a critical mass of early adopters is necessary for a new practice to “take off.”16 Thus the first challenge facing the profession is to identify, reach and support those early adopters. These are the leaders of professional associations, local dental societies, journal clubs and other well-respected members of the profession. Their visible support for tobacco cessation and willingness to serve as role models, mentors and promoters are critical to moving this issue along. Preparing the next generation of dentists is also essential. Adding TCS to dental curricula at the undergrad uate level will ensure future clinicians have the necessary knowledge and skills to deal with this issue. Provincial associations can encourage TCS adoption by including tobacco cessation as part of the standard of acceptable practice. Providing continuing education programs and credits will help ensure a competent workforce. It is also important to work in collaboration with the hygienist and assistant associations. Their skills in patient education and in preventive services are an integral part of successful TCS. The Alberta study would not have succeeded without the endorsement and collaboration of the dental, hygiene and assistant associations. Their involvement, advice and participation lent credibility to the project and was a key factor in many offices’ decision to participate. Preventing diseases like periodontitis, leukoplakia and oral cancers is not the purview of a single profession — indeed a team approach is essential for patient care.
The CDA has shown its leadership and commitment to improving oral health by
featuring tobacco cessation during dental health month. As the new millennium
progresses, it is up to individual dentists to show their commitment to better
oral health by incorporating TCS into their practice.
Acknowledgments: The Alberta Dental Study was funded by the National Cancer Institute of Canada with money raised by Canadian Cancer Society volunteers. We are especially grateful to Dr. Gordon Thompson of the Alberta Dental Association for his enthusiasm and support and to the Alberta Dental Hygienists Association and the Alberta Dental Assistants’ Association for their close collaboration. Without the support of these organizations this study would not have been possible.
Dr. Campbell is associate professor at the Centre for Behavioural Research and Program Evaluation, University of Waterloo.
Mrs. Simpson is principal consultant with Arden Research.
Dr. Petty is division head, department of dentistry and oral medicine, Calgary Regional Health Authority.
Dr. Jennett is a professor in the faculty of medicine, University of Calgary.
Correspondence to: Dr. H. Sharon Campbell, Centre for Behavioural Research and Program Evaluation, Lyle S. Hallman Institute, University of Waterloo, 200 University Ave. W., Waterloo, ON N2L 3G1. E-mail: sharoncm@healthy.uwaterloo.ca
The authors have no declared financial interest.
The views expressed are those of the authors and do not necessarily reflect the opinions or official policies of the Canadian Dental Association.
References 1. Christen AG, McDonald JL, Christen JA. The impact of tobacco use and cessation on nonmalignant and precancerous oral and dental diseases and conditions. Indiana University School of Dentistry Monograph. Indianapolis: Indiana School of Dentistry; 1991.
2. Bergstrom J, Eliasson S, Dock J. Exposure to tobacco smoking and periodontal health. J Clin Periodontol 2000; 27(1):61-8.
3. Tomar SL, Asthma S. Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol 2000; 71(5):743-51.
4. Garcia RI, Krall EA, Vokonas PS. Periodontal disease and mortality from all causes in the VA Dental Longitudinal Study. Ann Periodontol 1998; 3(1):339-49.
5. Machtei EE, Hausmann E, Dunford R, Grossi S, Ho A, Davis G and others. Longitudinal study of predictive factors for periodontal disease and tooth loss. J Clin Periodontol 1999; 26(6):374-80.
6. Paidi S, Pack AR, Thomson WM. An example of measurement and reporting of periodontal loss of attachment (LOA) in epidemiological studies: smoking and periodontal tissue destruction. N Z Dent J 1999; 95(422):118-23.
7. Tonetti MS. Cigarette smoking and periodontal diseases: etiology and management of disease. Ann Periodontol 1998; 3(1):88-101.
8. Mirbod SM, Ahing SI. Tobacco-associated lesions of the oral cavity: Part I. Nonmalignant lesions. J Can Dent Assoc 2000; 66(5):252-6.
9. Mirbod SM, Ahing SI. Tobacco-associated lesions of the oral cavity: Part II. Malignant lesions. J Can Dent Assoc 2000; 66(5):308-11.
10. Position paper: tobacco use and the periodontal patient. Research, Science and Therapy Committee of the American Academy of Periodontology. J Periodontol 1999; 70(11):1419-27.
11. Campbell HS, Petty TL, Meadows LM, Simpson L, Jennett PA. Improving tobacco cessation services in rural dental offices - recruitment to a randomized controlled trial. Can J Community Dent 1997; 12(2):15-22.
12. Jennett PA, Henry S, Campbell HS, Simpson L, Husack JP. Assessing the readiness of dentists’ offices to adopt tobacco cessation activities. J Continuing Educ Health Profession 1998; 18:119-27.
13. Campbell HS, Sletten M, Petty TL. Patient perceptions of tobacco cessation services in dental offices. J Am Dent Assoc 1999; 130(2):219-26.
14. Prochaska JO, DiClemente CC, Velicer W, Rossi J. Standardized, individualized, interactive, and personalized self-help programs for smoking cessation. Health Psychol 1993; 12(5):399-405.
15. Whitelaw, S Baldwin S, Bunton R, Flynn D. The status of evidence and outcomes in Stages of Change research. Health Educ Res 2000; 15(6):707-18.
16. Rogers EM. Diffusion of innovations. 4th ed. New York: The Free Press; 1995.
{kind=link}