35
Volume3 Issue1
|
S
upporting
Y
our
P
ractice
thirdof canals.Whereas first generationNiTi
rotaryfilesweredevelopedwithaconstant
taper suchas 0.04 (4%) or 0.06 (6%),
3
thenewer
generationsofNiTi rotary instrumentshave
beendesignedwithvariable tapers along
onefile. A fewexamplesof these instruments
arePROTAPERNEXT®,WaveOne®GOLDand
TRUShape® (DENTSPLYTulsaDental Specialties,
Tulsa, OK). TheV-Taper™RotarySystem (SS
White®, Lakewood, NJ) alsoaims toconserve
root dentin.
Conservative preparation of apical root
dentin
Moreconservativeand less tapered root canal
preparations seem tobe the key to reducing
catastrophic fractures inendodontically treated
teeth. However, larger apical preparations
could improve irrigationanddebris removal
fromcritical regionsof canals.
4,5
MostNiTi
instrumentshavebeendesignedwith this
concept inmind. Nevertheless, optimal apical
enlargement remains acontroversial topic.
Other considerations
Theamountof remaining tooth structure,
thoughcritical, isonlyoneof several factors
affecting the fracturepredilection inendodon-
tically treated teeth. Thechoiceof restoration
(posts, coresandcoronal coverage)
isequally important.Other factors that can
affect the fracture resistance include theendo-
dontic irrigant andmedicamentusedduring
treatment. Intra-canal bacteriacanalso induce
degradationofdentinal collagen, affectingden-
tinal strength.Moreover, age-relateddentinal
changeshavebeen shown toadverselyaffect
the strengthand toughnessofdentin.
6
Ultimately, it is theclinician’sdecision tomodify
hisor her conventional approach toendodon-
ticaccess andcanal preparation. Implementing
conservativeendodontic treatment approach-
es inone’sdailyendodonticpractice should
onlybeundertakenonce there is aclear understandingof theadvantages and
limitationsof thesenew techniques.
a
THEAUTHORS
Dr.MaryDabuleanu
Dr.Dabuleanu is an
endodontist in private
practice inNorthYork,
Ontario
Dr.GevikMalkhassian
Dr.Malkhassian is
anassistant professor
in endodontics at the
University ofToronto.He
is in endodontic private
practice inTorontoand
Mississauga.
Dr.SuhamAlexander
Dr.Alexander is in private
practice inOttawaand is
a clinical editor forOasis
Discussions atCDA.
Needexpertadvice?Send
usyourclinicalquestions.
or
1-855-71-OASIS
References
1.McCombD. RestorationoftheEndodonticallyTreatedTooth.Dispatch.February/March2008.
2.ClarkD,KhademiJ,HerbransonE.TheNewScienceofStrongEndoTeeth.DentistryToday,April9;2013.
3.TorabinejadM, FouadAWaltonR(2014)Endodontic Instruments inEndodonticsPrinciplesandPractice5thEd(pp:471-502). StLouis,
Missouri:Elsevier Inc.
4.KhademiA,YazdizadehM,FeizianfardM.DeterminationoftheMinimum InstrumentationSize forPenetrationof IrrigantstotheApical
ThirdofRootCanalSystems.JEndod.2006;32(5):417-420.
5.BoutsioukisC,LambrianidisT,VerhaagenB,VersluisM,KastrinakisE,WesselinkP,VanderSluisL.TheEffectofNeedle-insertionDepthon
the IrrigantFlow intheRootCanal:EvaluationUsinganUnsteadyComputationalFluidDynamicsModel.JEndod.2010;36:1664–1668.
6.KishenA.Mechanismsandrisk factors for fracturepredilection inendodonticallytreatedteeth.Endodontictopics2006,13,57-83.
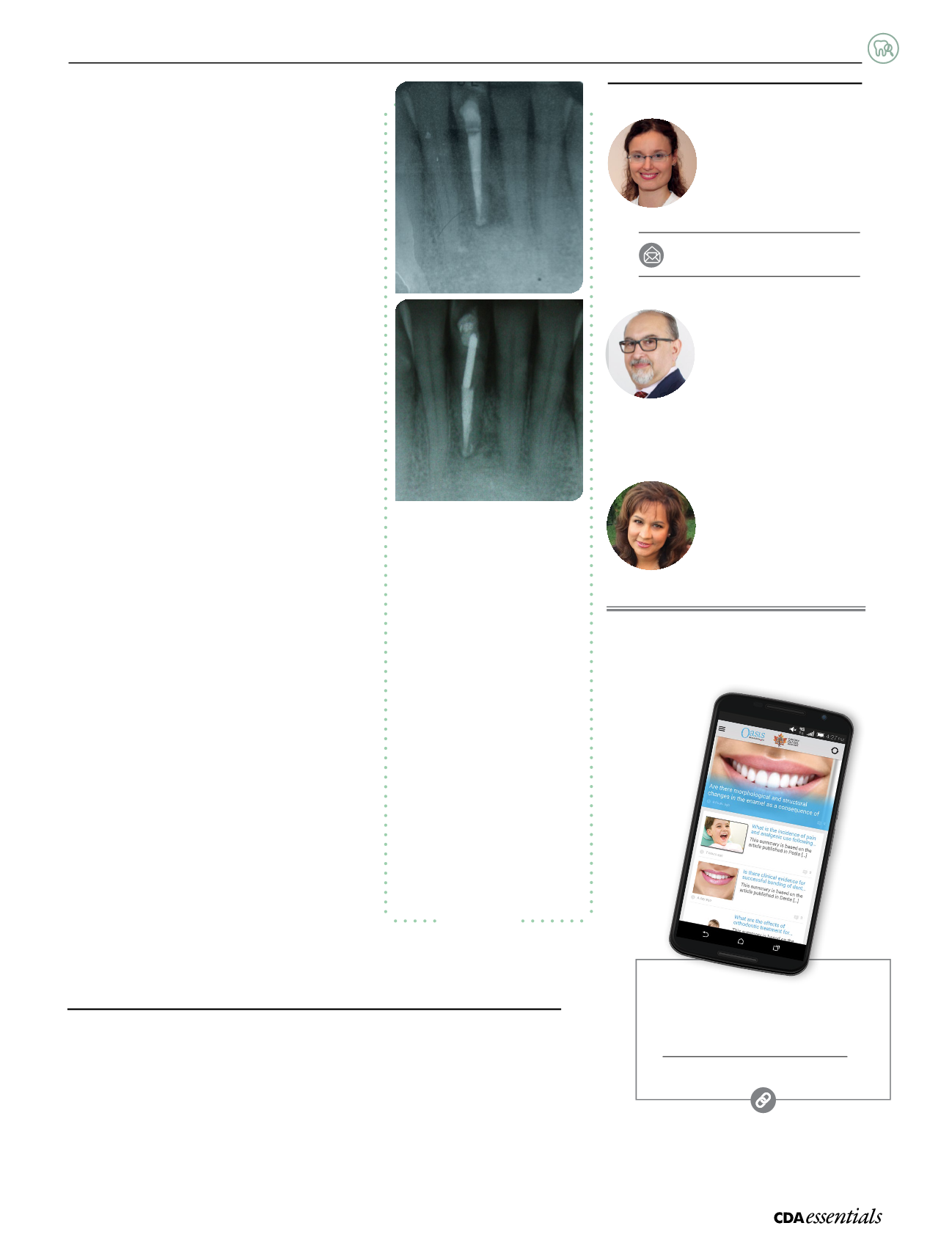
Radiographs illustratingacase in
whichendodontic treatmentwas
performedon tooth41and the
sequelae following treatment.
a)
Root canal treatment for tooth41
is complete.Note theexcessive
coronal taper thathasviolated the
PCD. Probingdepth is2–3mm
circumferentially.Note the
periapical lesionandheightof
thecrestal bone.
b)
Follow-up radiograph taken
5yearsafter completionof treat-
ment. Patient complainsofpain
tochewing.Note that theperiapical
lesionhashealedalmostcompletely.
However, anew J-shapedmesial
defect isevidenton tooth41 to the
apical extentof thepost. Thismesial
bone loss coincideswithanew
6-mmnarrowperiodontal pocket.
Onecan suspect that vertical root
fracturemighthaveoccurred
due toviolationof PCDandpost
placement. Tooth41 ishopelessand
extraction isadvised.
Figure2
a
b


